

Review
doi: 10.1093/bja/aeq299.
Lung protective strategies in anaesthesia
Affiliations
- PMID: 21148650
- PMCID: PMC9149602
- DOI: 10.1093/bja/aeq299
Item in Clipboard
Review
Lung protective strategies in anaesthesia
Br J Anaesth.
2010 Dec.
Abstract
Patients are at risk for several types of lung injury in the perioperative period including atelectasis, pneumonia, pneumothorax, acute lung injury, and acute respiratory distress syndrome. Anaesthetic management can cause, exacerbate, or ameliorate these injuries. This review examines the effects of perioperative mechanical ventilation and its role in ventilator-induced lung injury. Lung protective ventilatory strategies to specific clinical situations such as cardiopulmonary bypass and one-lung ventilation along with newer novel lung protective strategies are discussed.
Figures
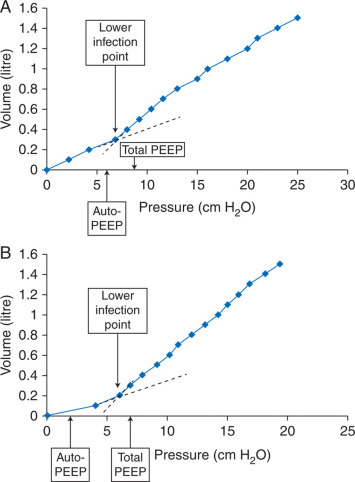
(a) An inspiratory compliance curve (lung volume vs airway pressure) during OLV as the lung is slowly inflated by 100 ml increments in a patient with mild COPD. The lower inflection point of the curve (thought to represent FRC) is at 7 cm H2O. During OLV, this patient developed intrinsic PEEP (measured by the end-expiratory airway occlusion plateau pressure ‘auto-PEEP’) of 6 cm H2O. The addition of 5 cm H2O of PEEP in this patient raised the end-expiratory lung volume above FRC, thus raising pulmonary vascular resistance in the ventilated lung and caused a deterioration in oxygenation. (b) The inspiratory compliance curve during OLV in a patient with normal pulmonary function. The lower inflection point of the curve is at 6 cm H2O. During OLV, this patient developed intrinsic PEEP of 2 cm H2O. The addition of 5 cm H2O of PEEP raised the end-expiratory lung volume to FRC, thus decreasing pulmonary vascular resistance in the ventilated lung and caused an improvement in oxygenation. Based on data from Slinger and colleagues.
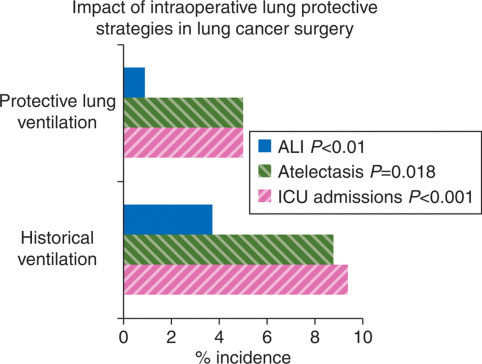
Impact of intraoperative lung protective strategies in lung cancer surgery. Comparison of historical control group vs lung protective ventilation group in patients undergoing OLV for lung cancer surgery showed significant benefits in terms of reduced ALI, atelectasis, and ICU admissions.
Similar articles
-
Mechanical ventilation with lung protective strategies: what works?Crit Care Clin. 2011 Jul;27(3):469-86. doi: 10.1016/j.ccc.2011.05.008. Crit Care Clin. 2011. PMID: 21742212 Review.
-
Contemporary ventilatory strategies for surgical patients.Semin Pediatr Surg. 2019 Feb;28(1):18-25. doi: 10.1053/j.sempedsurg.2019.01.004. Epub 2019 Jan 18. Semin Pediatr Surg. 2019. PMID: 30824129 Review.
-
Perioperative lung injury.Best Pract Res Clin Anaesthesiol. 2008 Mar;22(1):177-91. doi: 10.1016/j.bpa.2007.08.004. Best Pract Res Clin Anaesthesiol. 2008. PMID: 18494396 Review.
-
Perioperative lung protection strategies in cardiothoracic anesthesia: are they useful?Anesthesiol Clin. 2012 Dec;30(4):607-28. doi: 10.1016/j.anclin.2012.07.001. Epub 2012 Aug 2. Anesthesiol Clin. 2012. PMID: 23089498 Review.
-
Strategies to reduce ventilator-associated lung injury (VALI).Burns. 2013 Mar;39(2):200-11. doi: 10.1016/j.burns.2012.10.013. Epub 2012 Nov 24. Burns. 2013. PMID: 23183376 Review.
Cited by
-
Airway driving pressure is associated with postoperative pulmonary complications after major abdominal surgery: a multicentre retrospective observational cohort study.BJA Open. 2022 Dec;4:100099. doi: 10.1016/j.bjao.2022.100099. Epub 2022 Oct 18. BJA Open. 2022. PMID: 36687665 Free PMC article.
-
The effect of low versus high tidal volume ventilation on inflammatory markers in healthy individuals undergoing posterior spine fusion in the prone position: a randomized controlled trial.J Clin Anesth. 2012 Jun;24(4):263-9. doi: 10.1016/j.jclinane.2011.08.003. Epub 2011 Oct 15. J Clin Anesth. 2012. PMID: 22001758 Free PMC article. Clinical Trial.
-
Applications of pressure control ventilation volume guaranteed during one-lung ventilation in thoracic surgery.Int J Clin Exp Med. 2014 Apr 15;7(4):1094-8. eCollection 2014. Int J Clin Exp Med. 2014. PMID: 24955188 Free PMC article.
-
Pulmonary Complications following Percutaneous Nephrolithotomy: A Prospective Study.Curr Urol. 2013 Feb;7(3):113-6. doi: 10.1159/000356260. Epub 2014 Feb 10. Curr Urol. 2013. PMID: 24917770 Free PMC article.
-
Effects of alveolar recruitment maneuver on end-expiratory lung volume during one-lung ventilation.J Anesth. 2020 Apr;34(2):224-231. doi: 10.1007/s00540-019-02723-4. Epub 2019 Dec 17. J Anesth. 2020. PMID: 31848705
References
-
- Bendixen HH, Hedley-White J, Laver MB. Impaired oxygenation in surgical patients during general anesthesia with controlled ventilation: a concept of atelectasis. N Engl J Med. 1963;96:156–166. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
