

The role of trauma scoring in developing trauma clinical governance in the Defence Medical Services
- PMID: 21149354
- PMCID: PMC3013430
- DOI: 10.1098/rstb.2010.0232
The role of trauma scoring in developing trauma clinical governance in the Defence Medical Services
Abstract
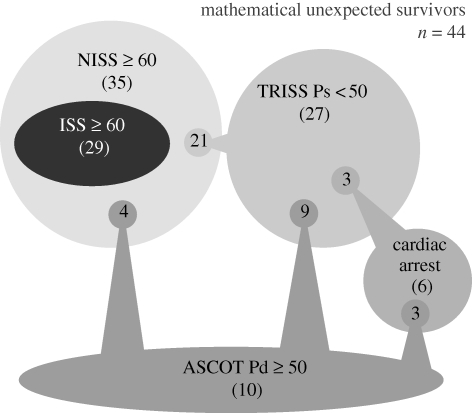
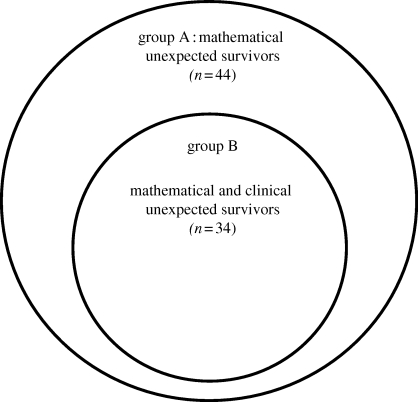
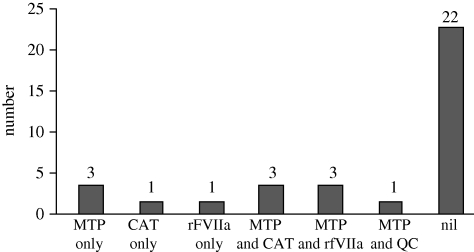
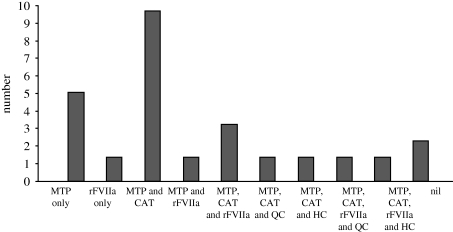
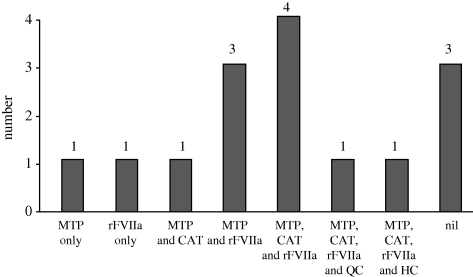
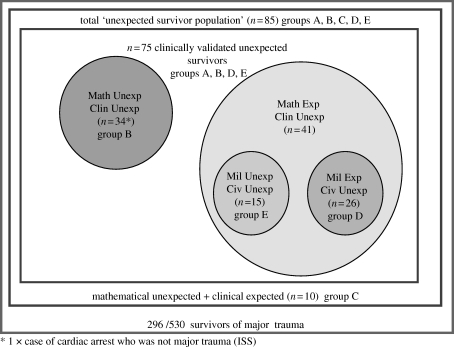
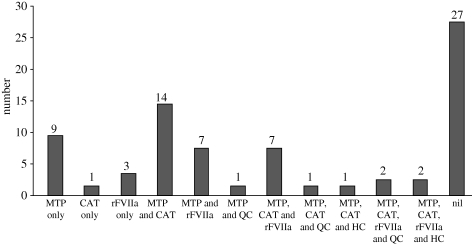
This paper discusses mathematical models of expressing severity of injury and probability of survival following trauma and their use in establishing clinical governance of a trauma system. There are five sections: (i) Historical overview of scoring systems--anatomical, physiological and combined systems and the advantages and disadvantages of each. (ii) Definitions used in official statistics--definitions of 'killed in action' and other categories and the importance of casualty reporting rates and comparison across conflicts and nationalities. (iii) Current scoring systems and clinical governance--clinical governance of the trauma system in the Defence Medical Services (DMS) by using trauma scoring models to analyse injury and clinical patterns. (iv) Unexpected outcomes--unexpected outcomes focus clinical governance tools. Unexpected survivors signify good practice to be promulgated. Unexpected deaths pick up areas of weakness to be addressed. Seventy-five clinically validated unexpected survivors were identified over 2 years during contemporary combat operations. (v) Future developments--can the trauma scoring methods be improved? Trauma scoring systems use linear approaches and have significant weaknesses. Trauma and its treatment is a complex system. Nonlinear methods need to be investigated to determine whether these will produce a better approach to the analysis of the survival from major trauma.
Figures
References
-
- SGPL 09/00 2000. Clinical governance in the Defence Medical Services. London, UK: Ministry of Defence
-
- SGPL 01/03 2003. Clinical governance in the Defence Medical Services. London, UK: Ministry of Defence
-
- SGPL 18/04 2004. Quality assurance of clinical governance on deployed operations. London, UK: Ministry of Defence
-
- Hodgetts T. J., Davies S., Russell R. J., McLeod J. 2007. Benchmarking the UK military deployed trauma system. J. R. Army Med. Corps 153, 237–238 - PubMed
-
- Smith J., Hodgetts T. J., Mahoney P. F., Russell R. J., Davies S., McLeod J. 2007. Trauma governance in the UK Defence Medical Services. J. R. Army Med. Corps 153, 239–242 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical