

Traumatic brain injury
- PMID: 21149359
- PMCID: PMC3013429
- DOI: 10.1098/rstb.2010.0230
Traumatic brain injury
Abstract
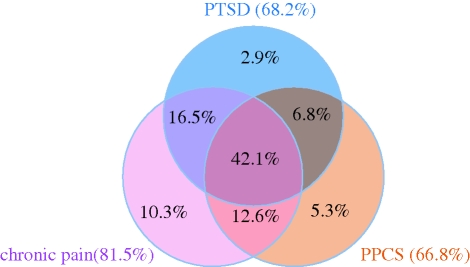
There is an increasing incidence of military traumatic brain injury (TBI), and similar injuries are seen in civilians in war zones or terrorist incidents. Indeed, blast-induced mild TBI has been referred to as the signature injury of the conflicts in Iraq and Afghanistan. Assessment involves schemes that are common in civilian practice but, in common with civilian TBI, takes little account of information available from modern imaging (particularly diffusion tensor magnetic resonance imaging) and emerging biomarkers. The efficient logistics of clinical care delivery in the field may have a role in optimizing outcome. Clinical care has much in common with civilian TBI, but intracranial pressure monitoring is not always available, and protocols need to be modified to take account of this. In addition, severe early oedema has led to increasing use of decompressive craniectomy, and blast TBI may be associated with a higher incidence of vasospasm and pseudoaneurysm formation. Visual and/or auditory deficits are common, and there is a significant risk of post-traumatic epilepsy. TBI is rarely an isolated finding in this setting, and persistent post-concussive symptoms are commonly associated with post-traumatic stress disorder and chronic pain, a constellation of findings that has been called the polytrauma clinical triad.
Figures

References
-
- Wolf S. J., Bebarta V. S., Bonnett C. J., Pons P. T., Cantrill S. V. 2009. Blast injuries. Lancet 374, 405–415 (doi:10.1016/S0140-6736(09)60257-9) - DOI - PubMed
-
- Maiden N. 2009. Ballistics reviews: mechanisms of bullet wound trauma. Forensic Sci. Med. Pathol. 5, 204–209 (doi:10.1007/s12024-009-9096-6) - DOI - PubMed
-
- Jandial R., Reichwage B., Levy M., Duenas V., Sturdivan L. 2008. Ballistics for the neurosurgeon. Neurosurgery 62, 472–480 (doi:10.1227/01.neu.0000316015.05550.7a) - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials