

Review
doi: 10.1098/rstb.2010.0214.
End-to-end military pain management
Affiliations
- PMID: 21149362
- PMCID: PMC3013425
- DOI: 10.1098/rstb.2010.0214
Item in Clipboard
Review
End-to-end military pain management
Philos Trans R Soc Lond B Biol Sci.
.
Abstract
The last three years have seen significant changes in the Defence Medical Services approach to trauma pain management. This article seeks to outline these changes that have occurred at every level of the casualty's journey along the chain of evacuation, from the point of injury to rehabilitation and either continued employment in the Services or to medical discharge. Particular attention is paid to the evidence for the interventions used for both acute pain and chronic pain management. Also highlighted are possible differences in pain management techniques between civilian and military casualties.
Figures
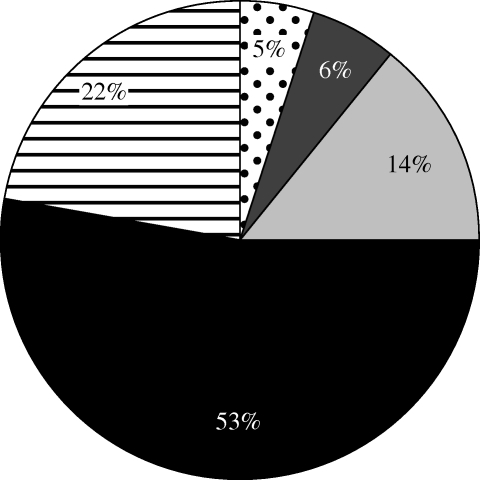
A pie chart indicating the distribution of pain scores at the point of wounding as remembered by casualties (pain scores: dotted region, none; dark grey region, mild; light grey region, moderate; black region, severe; hatched region, do not remember).
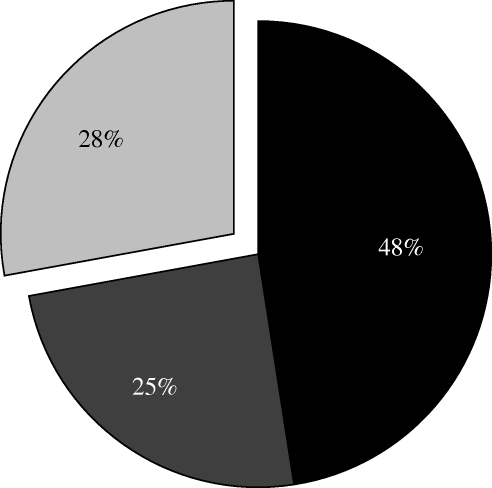
A pie chart representing the distribution of responses given when casualties were asked to remember whether their initial analgesia helped to relieve their pain (responses: black region, yes; dark grey region, no; light grey region, do not remember).
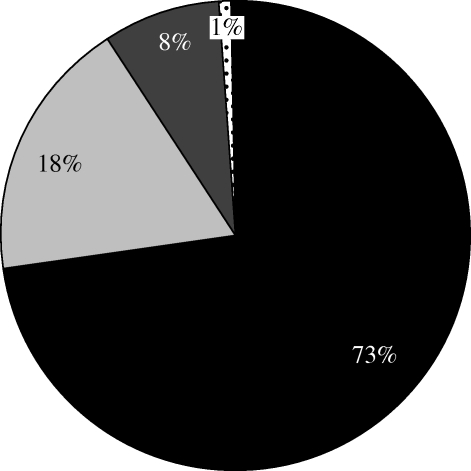
A pie chart demonstrating the distribution of pain scores recorded among the military patients at RCDM over five weeks. There were 922 data points (pain score: black region, 0; light grey region, 1; dark grey region, 2; dotted region, 3).
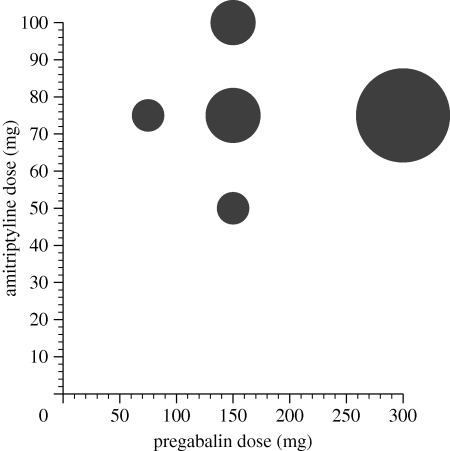
The typical doses of amitriptyline taken at night and pregabalin taken twice a day used by the military casualties at RCDM. The size of the data point is proportional to the number of patients on that combination, so most are on 75 mg amitriptyline (at night) and 300 mg pregabalin (twice a day).
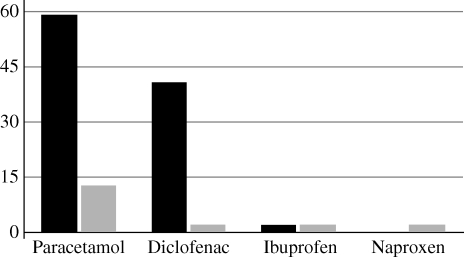
The differences between the percentage of amputees taking simple analgesics when they initially presented at DMRC and the last entry in their notes (black bars, % initially; grey bars, % finally).
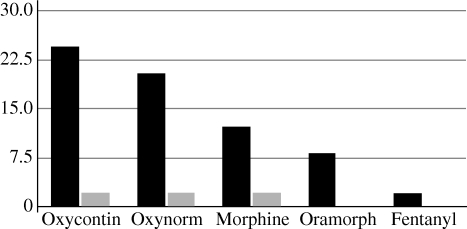
The differences between the percentage of amputees taking strong opioids when they initially presented at DMRC and the last entry in their notes (black bars, % initially; grey bars, % finally).
References
-
- Sir Liam Donaldson C.M.O. 2009. 150 years of the annual report of the Chief Medical Officer: on the state of public health 2008. pp. 73 London, UK: Department of Health
-
- Cousins M., Power I. 1994. Acute and postoperative pain. In Textbook of pain (eds Melzack R., Wall P. D.), pp. 357–385 London, UK: Churchill Livingstone
-
- Holbrook T. L., Galarneau M. R., Dye J. L., Quinn K., Dougherty A. L. 2010. Morphine use after combat injury in Iraq and post-traumatic stress disorder. N. Engl. J. Med. 362, 110–117 (doi:10.1056/NEJMoa0903326) - DOI - PubMed
-
- Merskey H., Bogduk N. 1994. Classification of chronic pain (eds Merskey H., Bogduk N.). Seattle: International Association for the Study of Pain
-
- Tracey I., Bushnell M. C. 2009. How neuroimaging studies have challenged us to rethink: is chronic pain a disease? J. Pain 10, 1113–1120 (doi:10.1016/j.jpain.2009.09.001) - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical