

Validation of consensus panel diagnosis in dementia
- PMID: 21149812
- PMCID: PMC3178413
- DOI: 10.1001/archneurol.2010.301
Validation of consensus panel diagnosis in dementia
Abstract
Background: The clinical diagnosis of dementing diseases largely depends on the subjective interpretation of patient symptoms. Consensus panels are frequently used in research to determine diagnoses when definitive pathologic findings are unavailable. Nevertheless, research on group decision making indicates that many factors can adversely affect panel performance.
Objective: To determine conditions that improve consensus panel diagnosis.
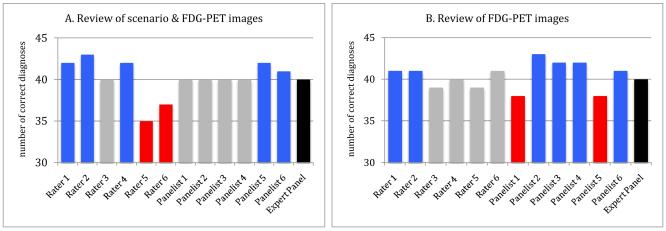
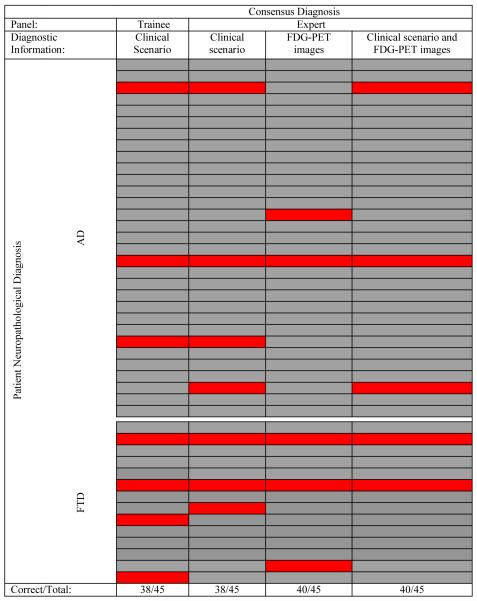
Design: Comparison of neuropathologic diagnoses with individual and consensus panel diagnoses based on clinical scenarios only, fludeoxyglucose F 18 positron emission tomography images only, and scenarios plus images.
Setting: Expert and trainee individual and consensus panel deliberations using a modified Delphi method in a pilot research study of the diagnostic utility of fludeoxyglucose F 18 positron emission tomography.
Patients: Forty-five patients with pathologically confirmed Alzheimer disease or frontotemporal dementia.
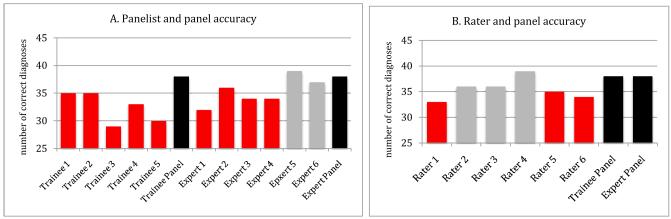
Main outcome measures: Statistical measures of diagnostic accuracy, agreement, and confidence for individual raters and panelists before and after consensus deliberations.
Results: The consensus protocol using trainees and experts surpassed the accuracy of individual expert diagnoses when clinical information elicited diverse judgments. In these situations, consensus was 3.5 times more likely to produce positive rather than negative changes in the accuracy and diagnostic certainty of individual panelists. A rule that forced group consensus was at least as accurate as majority and unanimity rules.
Conclusions: Using a modified Delphi protocol to arrive at a consensus diagnosis is a reasonable substitute for pathologic information. This protocol improves diagnostic accuracy and certainty when panelist judgments differ and is easily adapted to other research and clinical settings while avoiding the potential pitfalls of group decision making.
Figures
References
-
- Ott A, Stolk RP, van Harskamp F, Pols HA, Hofman A, Breteler MM. Diabetes mellitus and the risk of dementia: The Rotterdam Study. Neurology. 1999;53(9):1937–1942. - PubMed
-
- Lopez OL, Becker JT, Klunk W, et al. Research evaluation and diagnosis of probable Alzheimer’s disease over the last two decades: I. Neurology. 2000;55(12):1854–1862. - PubMed
-
- Shekelle PG, Kahan JP, Bernstein SJ, Leape LL, Kamberg CJ, Park RE. The reproducibility of a method to identify the overuse and underuse of medical procedures. N Engl J Med. 1998;338(26):1888–1895. - PubMed
-
- Huttin C. The use of clinical guidelines to improve medical practice: main issues in the United States. Int J Qual Health Care. 1997;9(3):207–214. - PubMed
-
- Gabel MJ, Shipan CR. A social choice approach to expert consensus panels. J Health Econ. 2004;23(3):543–564. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- P50 AG008671/AG/NIA NIH HHS/United States
- AG16573/AG/NIA NIH HHS/United States
- AG08671/AG/NIA NIH HHS/United States
- U01 AG016976/AG/NIA NIH HHS/United States
- AG0238377/AG/NIA NIH HHS/United States
- P50 AG016573/AG/NIA NIH HHS/United States
- AG05133/AG/NIA NIH HHS/United States
- P50 AG005133/AG/NIA NIH HHS/United States
- AG10129/AG/NIA NIH HHS/United States
- P30 AG010124/AG/NIA NIH HHS/United States
- AG10124/AG/NIA NIH HHS/United States
- P30 AG010133/AG/NIA NIH HHS/United States
- K23 AG030006/AG/NIA NIH HHS/United States
- AG12300/AG/NIA NIH HHS/United States
- P30 AG012300/AG/NIA NIH HHS/United States
- R01 AG022394/AG/NIA NIH HHS/United States
- AG16976/AG/NIA NIH HHS/United States
- AG10133/AG/NIA NIH HHS/United States
- AG22394/AG/NIA NIH HHS/United States
- P30 AG010129/AG/NIA NIH HHS/United States
