

Optimum time to start antiretroviral therapy during HIV-associated opportunistic infections
- PMID: 21150593
- PMCID: PMC3801096
- DOI: 10.1097/QCO.0b013e3283420f76
Optimum time to start antiretroviral therapy during HIV-associated opportunistic infections
Abstract
Purpose of review: We review recently published literature concerning the optimum time to start antiretroviral therapy (ART) in patients with HIV-associated opportunistic infections.
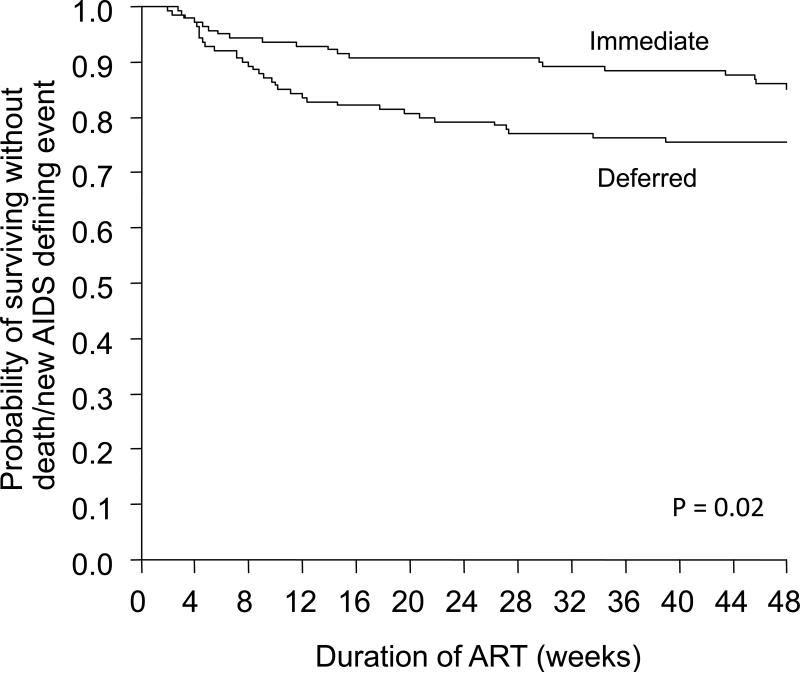
Recent findings: In addition to data from observational studies, results from six randomized controlled clinical trials were available by July 2010. The collective findings of these trials were that patients with CD4 cell counts less than 200 cells/μl who start ART within the first 2 weeks of treatment for opportunistic infections including Pneumocystis jirovecii pneumonia, serious bacterial infections or pulmonary tuberculosis have lower mortality when compared to patients starting ART at later time-points. Moreover, patients with pulmonary tuberculosis and CD4 counts of 200-500 cells/μl who started ART during tuberculosis (TB) treatment had improved survival compared to those who deferred ART until after the end of treatment. In contrast, in two separate studies, immediate ART conferred no survival benefit in patients with TB meningitis and was associated with substantially higher mortality risk in patients with cryptococcal meningitis.
Summary: Initiation of ART during the first 2 weeks of treatment for serious opportunistic infections has been shown to be associated with improved survival with the exception of patients with tuberculous meningitis and cryptococcal meningitis. Further clinical trials are ongoing.
Figures

References
-
- Egger M, May M, Chene G, et al. Prognosis of HIV-1-infected patients starting highly active antiretroviral therapy: a collaborative analysis of prospective studies. Lancet. 2002;360:119–29. - PubMed
-
- Braitstein P, Brinkhof MW, Dabis F, et al. Mortality of HIV-1-infected patients in the first year of antiretroviral therapy: comparison between low-income and high-income countries. Lancet. 2006;367:817–24. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
