

Impact on disease-free survival of adjuvant erlotinib or gefitinib in patients with resected lung adenocarcinomas that harbor EGFR mutations
- PMID: 21150674
- PMCID: PMC3778680
- DOI: 10.1097/JTO.0b013e318202bffe
Impact on disease-free survival of adjuvant erlotinib or gefitinib in patients with resected lung adenocarcinomas that harbor EGFR mutations
Abstract
Background: Patients with stage IV lung adenocarcinoma and epidermal growth factor receptor (EGFR) mutation derive clinical benefit from treatment with EGFR tyrosine kinase inhibitors (TKIs). Whether treatment with TKI improves outcomes in patients with resected lung adenocarcinoma and EGFR mutation is unknown.
Methods: Data were analyzed from a surgical database of patients with resected lung adenocarcinoma harboring EGFR exon 19 or 21 mutations. In a multivariate analysis, we evaluated the impact of treatment with adjuvant TKI.
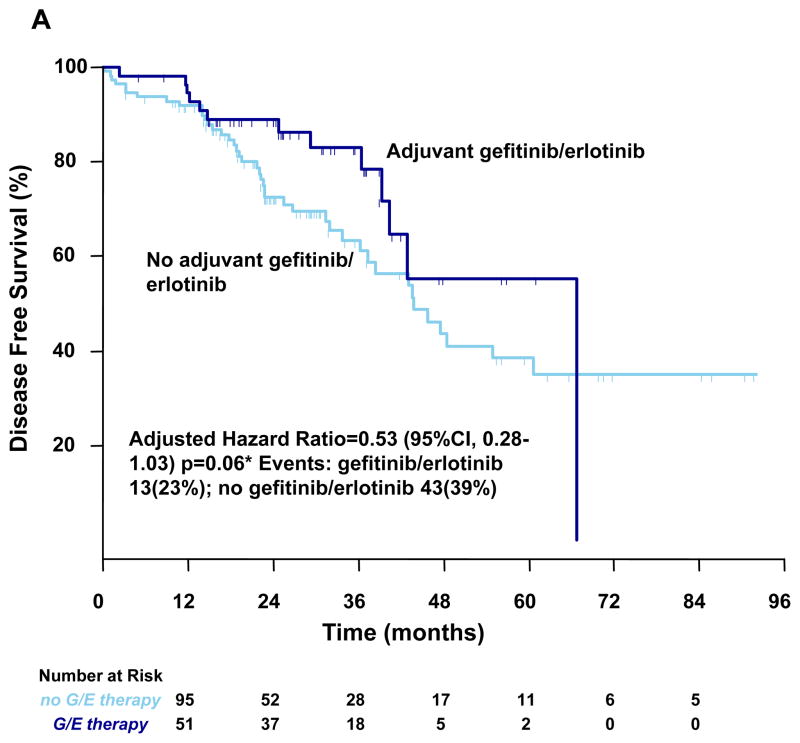
Results: The cohort consists of 167 patients with completely resected stages I to III lung adenocarcinoma. Ninety-three patients (56%) had exon 19 del, 74 patients (44%) had exon 21 mutations, and 56 patients (33%) received perioperative TKI. In a multivariate analysis controlling for sex, stage, type of surgery, and adjuvant platinum chemotherapy, the 2-year disease-free survival (DFS) was 89% for patients treated with adjuvant TKI compared with 72% in control group (hazard ratio = 0.53; 95% confidence interval: 0.28-1.03; p = 0.06). The 2-year overall survival was 96% with adjuvant EGFR TKI and 90% in the group that did not receive TKI (hazard ratio: 0.62; 95% confidence interval: 0.26-1.51; p = 0.296).
Conclusions: Compared with patients who did not receive adjuvant TKI, we observed a trend toward improvement in DFS among individuals with resected stages I to III lung adenocarcinomas harboring mutations in EGFR exon 19 or 21 who received these agents as adjuvant therapy. Based on these data, 320 patients are needed for a randomized trial to prospectively validate this DFS benefit.
Figures


References
-
- Ginsberg RJ, Rubinstein LV. Randomized trial of lobectomy versus limited resection for T1 N0 non-small cell lung cancer. Lung Cancer Study Group. Ann Thorac Surg. 1995;60:615–22. discussion 622–3. - PubMed
-
- Goldstraw P, Crowley J, Chansky K, et al. The IASLC Lung Cancer Staging Project: proposals for the revision of the TNM stage groupings in the forthcoming (seventh) edition of the TNM Classification of malignant tumours. J Thorac Oncol. 2007;2:706–14. - PubMed
-
- Douillard JY, Rosell R, De Lena M, et al. Adjuvant vinorelbine plus cisplatin versus observation in patients with completely resected stage IB-IIIA non-small-cell lung cancer (Adjuvant Navelbine International Trialist Association [ANITA]): a randomised controlled trial. Lancet Oncol. 2006;7:719–27. - PubMed
-
- Winton T, Livingston R, Johnson D, et al. Vinorelbine plus cisplatin vs. observation in resected non-small-cell lung cancer. N Engl J Med. 2005;352:2589–97. - PubMed
-
- Arriagada R, Bergman B, Dunant A, et al. Cisplatin-based adjuvant chemotherapy in patients with completely resected non-small-cell lung cancer. N Engl J Med. 2004;350:351–60. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
