

What is the malignant nature of human ductal carcinoma in situ?
- PMID: 21150936
- PMCID: PMC3756606
- DOI: 10.1038/nrc2950
What is the malignant nature of human ductal carcinoma in situ?
Abstract
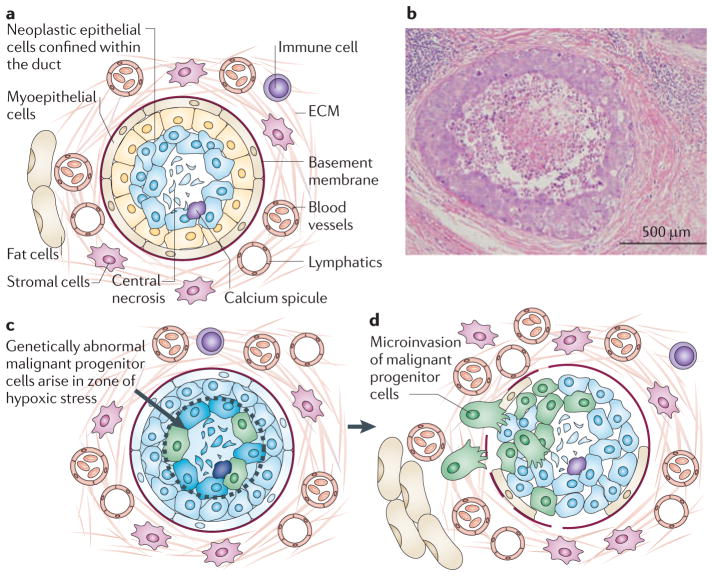
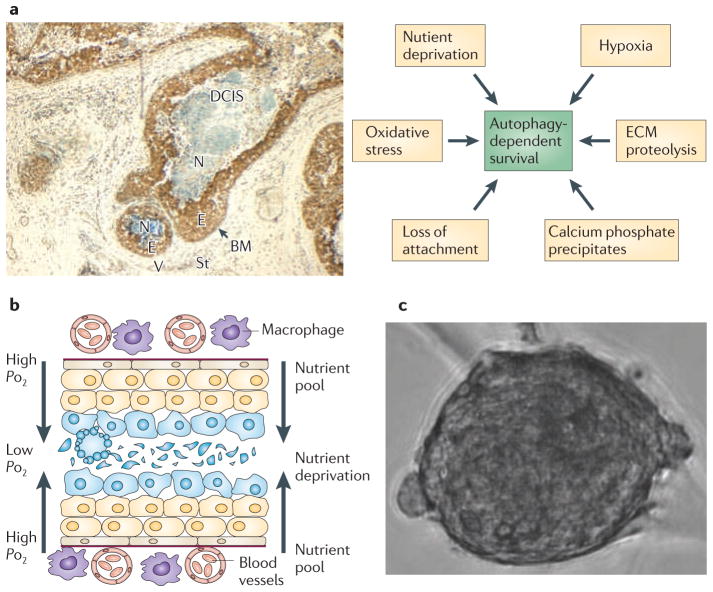
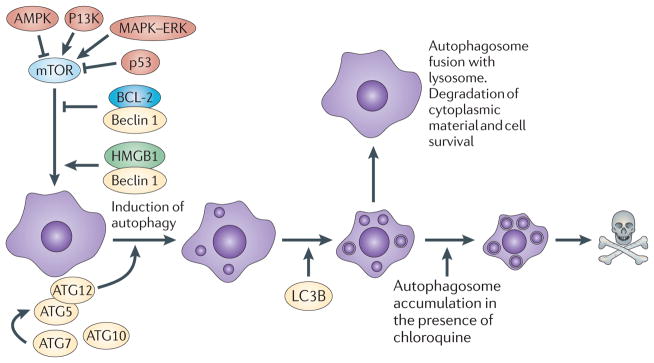
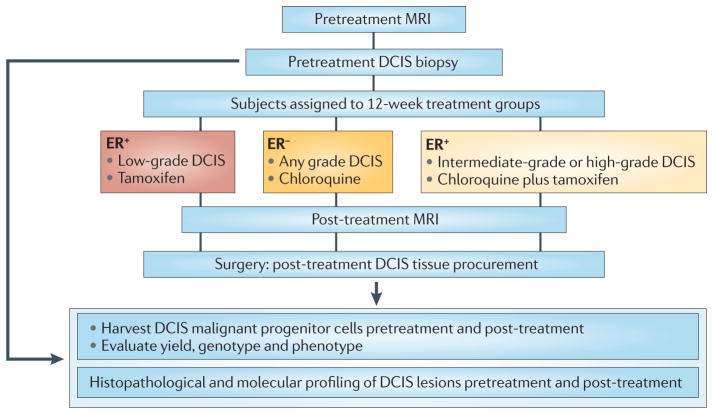
Invasive, genetically abnormal carcinoma progenitor cells have been propagated from human and mouse breast ductal carcinoma in situ (DCIS) lesions, providing new insights into breast cancer progression. The survival of DCIS cells in the hypoxic, nutrient-deprived intraductal niche could promote genetic instability and the derepression of the invasive phenotype. Understanding potential survival mechanisms, such as autophagy, that might be functioning in DCIS lesions provides strategies for arresting invasion at the pre-malignant stage. A new, open trial of neoadjuvant therapy for patients with DCIS constitutes a model for testing investigational agents that target malignant progenitor cells in the intraductal niche.
Conflict of interest statement
The authors declare no competing financial interests.
Figures
Comment in
-
The two faces of autophagy and the pathological underestimation of DCIS.Nat Rev Cancer. 2011 Jul 22;11(8):618; author reply 618. doi: 10.1038/nrc2950-c1. Nat Rev Cancer. 2011. PMID: 21779013 No abstract available.
References
-
- Allegra C, et al. NIH state-of-the-science conference statement: diagnosis and management of ductal carcinoma in situ. NIH Consens State Sci Statements. 2009;26:1–27. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
