

Human Lymphatic Architecture and Dynamic Transport Imaged Using Near-infrared Fluorescence
- PMID: 21151475
- PMCID: PMC3000461
- DOI: 10.1593/tlo.10190
Human Lymphatic Architecture and Dynamic Transport Imaged Using Near-infrared Fluorescence
Abstract
Background: Although the importance of lymphatic function is well recognized, the lack of real-time imaging modalities limits our understanding of its role in many diseases. In a phase 0 exploratory study, we used dynamic, near-infrared (NIR) fluorescence imaging to assess the extremes of lymphatic architecture and transport in healthy human subjects and in subjects clinically diagnosed with unilateral lymphedema (LE), a disease that can be prevalent in cancer survivors.
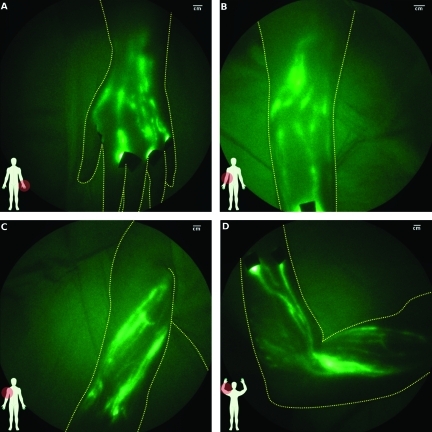
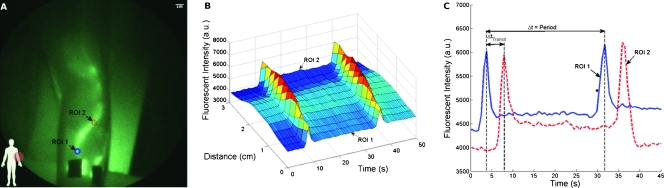
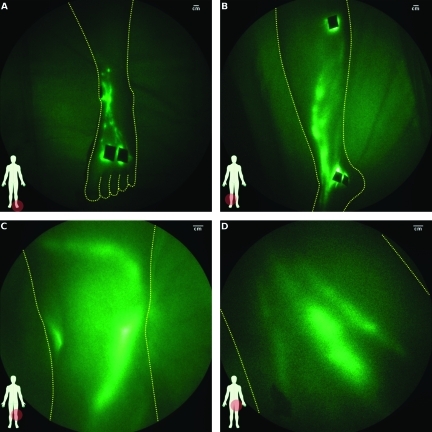
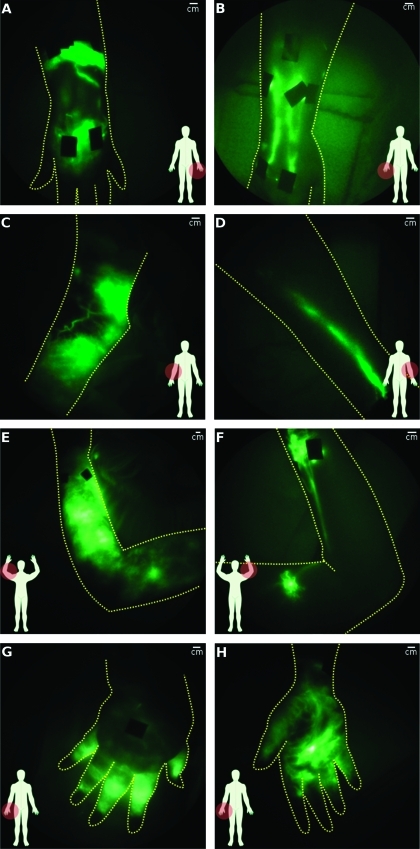
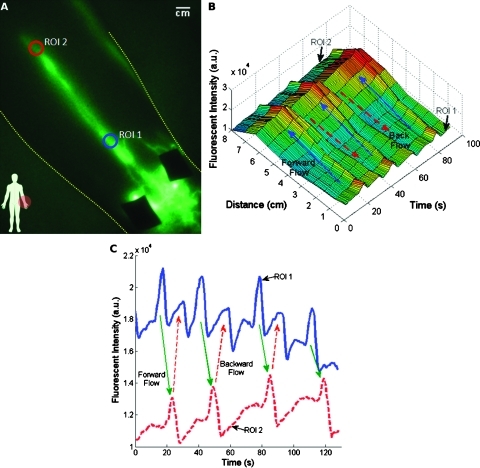
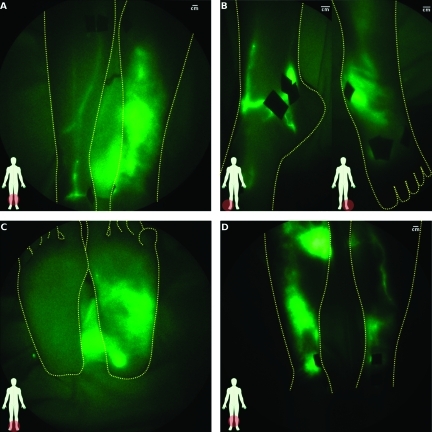
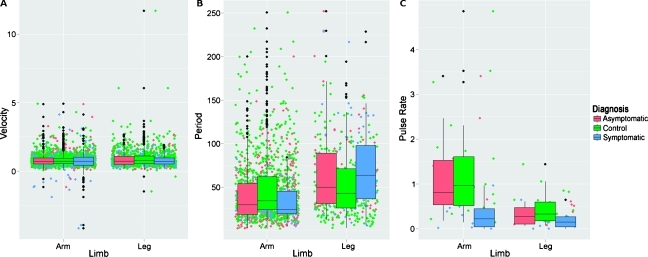
Methods and results: Active lymphatic propulsion was imaged after intradermal injections of 25 µg of indocyanine green (total maximum dose ≤400 µg) bilaterally in the arms or legs of control and subjects. Images show well-defined lymphatic structures with propulsive dye transport in limbs of healthy subjects. In LE subjects, we observed extravascular dye accumulation, networks of fluorescent lymphatic capillaries, and/or tortuous lymphatic vessels in all symptomatic and some asymptomatic limbs. Statistical models indicate that disease status and/or limb significantly affect parameters of apparent lymph propagation velocity and contractile frequency.
Conclusions: These clinical research studies demonstrate the potential of NIR fluorescence imaging as a diagnostic measure of functional lymphatics and as a new tool in translational research studies to decipher the role of the lymphatic system in cancer and other diseases.
Figures
References
-
- Swartz MA. The physiology of the lymphatic system. Adv Drug Deliv Rev. 2001;50(1–2):3–20. - PubMed
-
- Sakorafas GH, Peros G, Cataliotti L, Vlastos G. Lymphedema following axillary lymph node dissection for breast cancer. Surg Oncol. 2006;15(3):153–165. - PubMed
-
- Farncombe M, Daniels G, Cross L. Lymphedema—the seemingly forgotten complication. J Pain Symptom Manage. 1994;9(4):269–276. - PubMed
-
- Rockson SG. Lymphedema. Am J Med. 2001;110(4):288–295. - PubMed
-
- Ridner SH. Pretreatment lymphedema education and identified educational resources in breast cancer patients. Patient Educ Couns. 2006;61(1):72–79. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous