

Bone impairment in phenylketonuria is characterized by circulating osteoclast precursors and activated T cell increase
- PMID: 21152388
- PMCID: PMC2994752
- DOI: 10.1371/journal.pone.0014167
Bone impairment in phenylketonuria is characterized by circulating osteoclast precursors and activated T cell increase
Abstract
Background: Phenylketonuria (PKU) is a rare inborn error of metabolism often complicated by a progressive bone impairment of uncertain etiology, as documented by both ionizing and non- ionizing techniques.
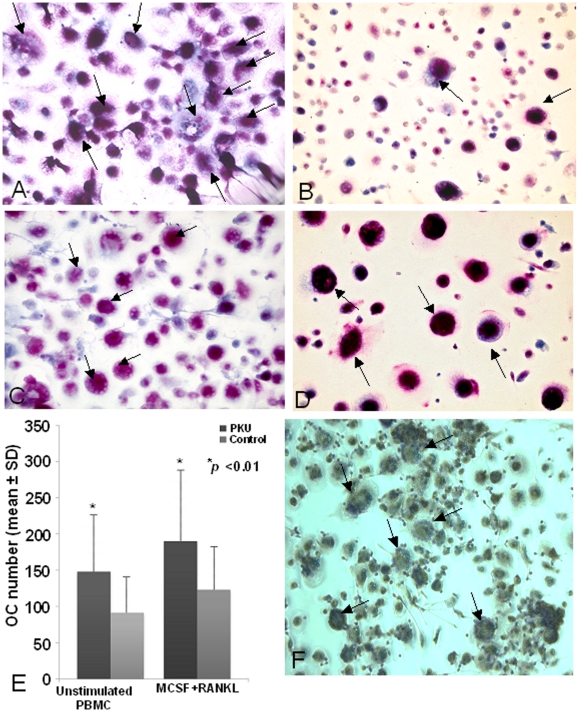
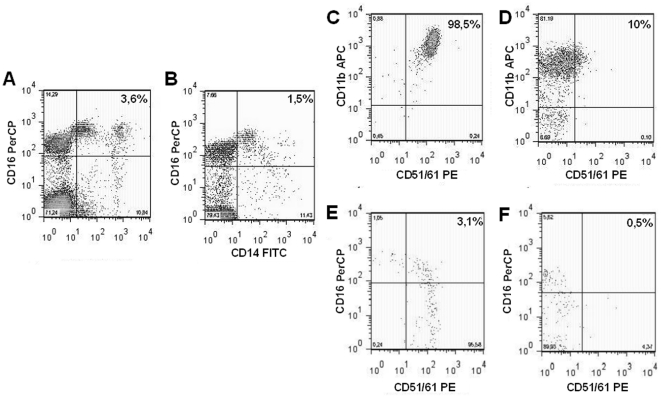
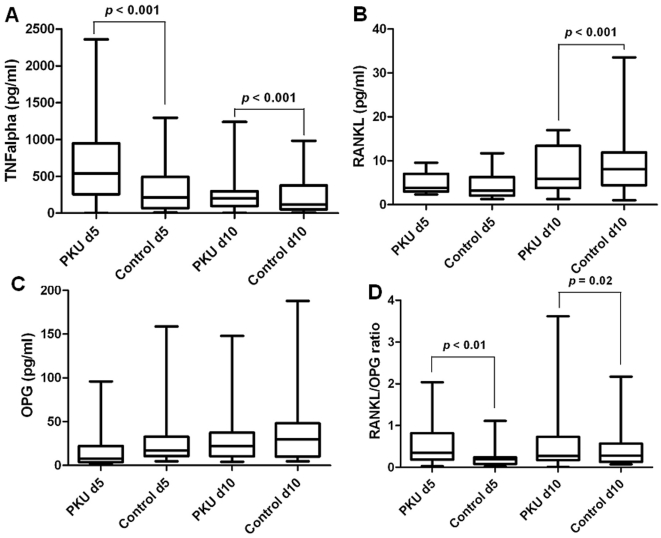
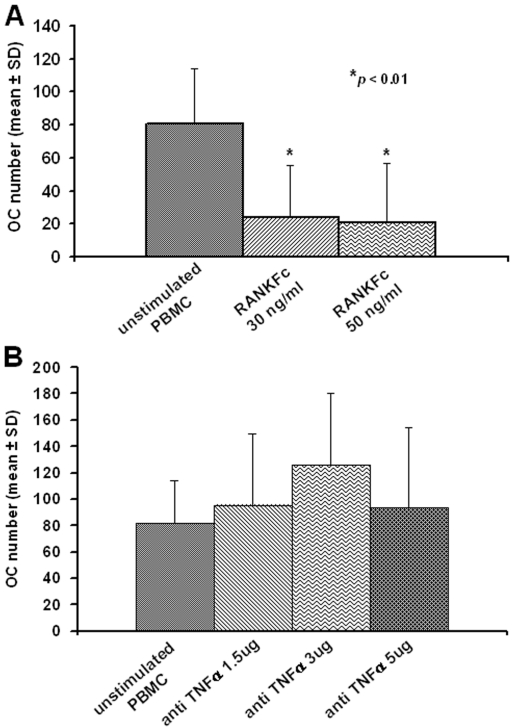
Methodology: Peripheral blood mononuclear cell (PBMC) cultures were performed to study osteoclastogenesis, in the presence or absence of recombinant human monocyte-colony stimulating factor (M-CSF) and receptor activator of NFκB ligand (RANKL). Flow cytometry was utilized to analyze osteoclast precursors (OCPs) and T cell phenotype. Tumour necrosis factor α (TNF-α), RANKL and osteoprotegerin (OPG) were quantified in cell culture supernatants by ELISA. The effects of RANKFc and anti-TNF-α antibodies were also investigated to determine their ability to inhibit osteoclastogenesis. In addition, bone conditions and phenylalanine levels in PKU patients were clinically evaluated.
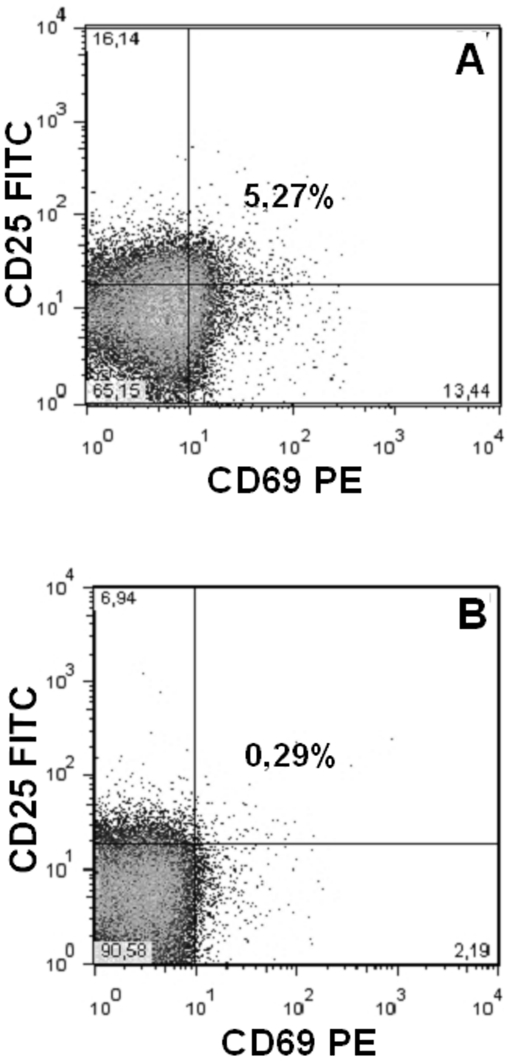
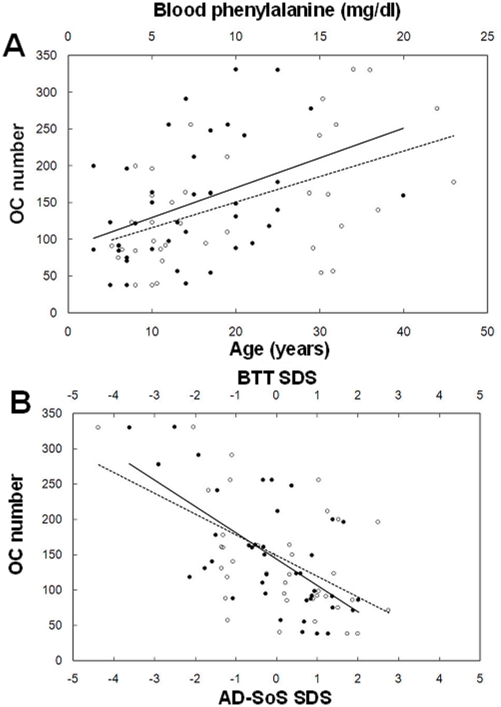
Principal findings: Several in vitro studies in PKU patients' cells identified a potential mechanism of bone formation inhibition commonly associated with this disorder. First, PKU patients disclosed an increased osteoclastogenesis compared to healthy controls, both in unstimulated and M-CSF/RANKL stimulated PBMC cultures. OCPs and the measured RANKL/OPG ratio were higher in PKU patients compared to healthy controls. The addition of specific antagonist RANKFc caused osteoclastogenesis inhibition, whereas anti-TNF-α failed to have this effect. Among PBMCs isolated from PKU patients, activated T cells, expressing CD69, CD25 and RANKL were identified. Confirmatory in vivo studies support this proposed model. These in vivo studies included the analysis of osteoclastogenesis in PKU patients, which demonstrated an inverse relation to bone condition assessed by phalangeal Quantitative Ultrasound (QUS). This was also directly related to non-compliance to therapeutic diet reflected by hyperphenylalaninemia.
Conclusions: Our results indicate that PKU spontaneous osteoclastogenesis depends on the circulating OCP increase and the activation of T cells. Osteoclastogenesis correlates with clinical parameters, suggesting its value as a diagnostic tool for an early assessment of an increased bone resorption in PKU patients.
Conflict of interest statement
Figures
References
-
- Scriver C, Kaufman S. New York: McGraw-Hill; 2001. The Metabolic and Molecular Bases of Inherited Disease, ed. 8th. Vol. 2. 2001. pp. 1667–1724.
-
- Bickel H, Gerrard J, Hickmans EM. Influence of phenylalanine intake on phenylketonuria. Lancet. 1953;265(6790):812–3. - PubMed
-
- Hoeks MP, den Heijer M, Janssen MC. Adult issues in phenylketonuria. Neth J Med. 2009;67(1):2–7. - PubMed
-
- Allen JR, Humphries IR, Waters DL, Roberts DC, Lipson AH, et al. Decreased bone mineral density in children with phenylketonuria. Am J Clin Nutr. 1994;59(2):419–22. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
