

log(TG)/HDL-C is related to both residual cardiometabolic risk and β-cell function loss in type 2 diabetes males
- PMID: 21156040
- PMCID: PMC3020173
- DOI: 10.1186/1475-2840-9-88
log(TG)/HDL-C is related to both residual cardiometabolic risk and β-cell function loss in type 2 diabetes males
Abstract
Background: T2DM is associated with atherogenic dyslipidemia (AD), defined as decreased HDL-C plus raised triglycerides (TG). AD confers increased risk for CAD, even when LDL-C is at target. AD is rarely assessed due to lack of screening methods consensus.
Aim: To establish the prevalence and severity of AD from log(TG)/HDL-C in T2DM males, and to determine how it relates to cardiometabolic phenotype, glucose homeostasis, micro- and macrovascular complications, and 10-year UKPDS CV risk.
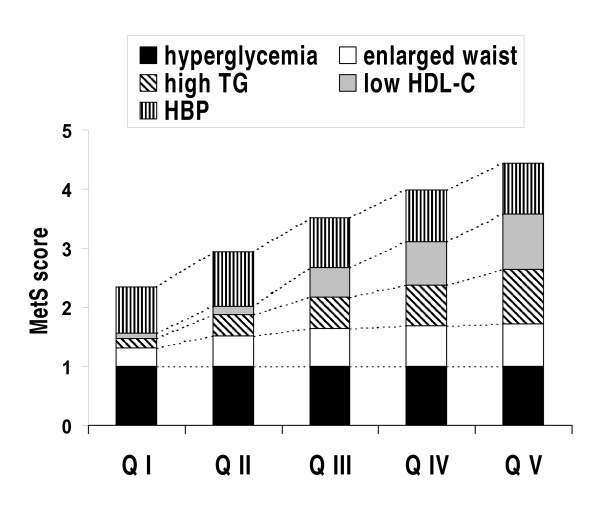
Methods: 585 T2DM males divided according to quintiles (Q) of log(TG)/HDL-C. AD prevalence defined as HDL-C <40 mg x dL(-1) plus TG ≥150 mg x dL(-1). β-cell function assessed with HOMA.
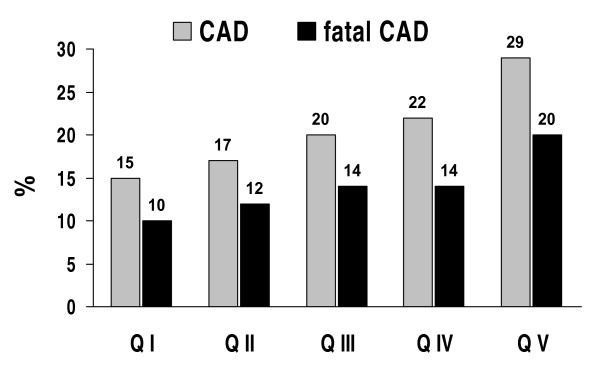
Results: Mean HDL-C and TG were 44 (13) and 204 (155) mg x dL(-1). AD prevalence was 35%. AD correlated with lower β-cell function, with accelerated loss of insulin secretion, and with poorer HbA1c levels. AD was related to a high prevalence of CAD, and also to 10-year absolute CAD risk.
Conclusions: log(TG)/HDL-C is a simple means to estimate AD and the residual CV risk it confers in T2DM. AD closely associates with major cardiometabolic and glucose homeostasis determinants and poorer metabolic control. The ratio also relates to macroangiopathy prevalence and ranks future CAD risk, and is well-suited to capture non-LDL-related macrovascular residual risk and major glycemic determinants.
Figures
References
-
- Brites FD, Bonavita CD, De Geitere C, Cloës M, Delfly B, Yael MJ, Fruchart J, Wikinski RW, Castro GR. Alterations in the main steps of reverse cholesterol transport in male patients with primary hypertriglyceridemia and low HDL-cholesterol levels. Atherosclerosis. 2000;152:181–92. doi: 10.1016/S0021-9150(99)00452-9. - DOI - PubMed
-
- Fruchart J-C, Sacks F, Hermans MP, Assmann G, Brown WV, Ceska R, Chapman MJ, Dodson PM, Fioretto P, Ginsberg HN, Kadowaki T, Lablanche J-M, Marx N, Plutzky J, Reiner Z, Rosenson RS, Staels B, Stock JK, Sy R, Wanner C, Zambon A, Zimmet P. for the Residual Risk Reduction Initiative. The Residual Risk Reduction Initiative: a call to action to reduce residual vascular risk in patients with dyslipidemia. Am J Cardiol. 2008;102:S1–34. doi: 10.1016/j.amjcard.2008.10.002. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
