

Does this older adult with lower extremity pain have the clinical syndrome of lumbar spinal stenosis?
- PMID: 21156951
- PMCID: PMC3260477
- DOI: 10.1001/jama.2010.1833
Does this older adult with lower extremity pain have the clinical syndrome of lumbar spinal stenosis?
Abstract
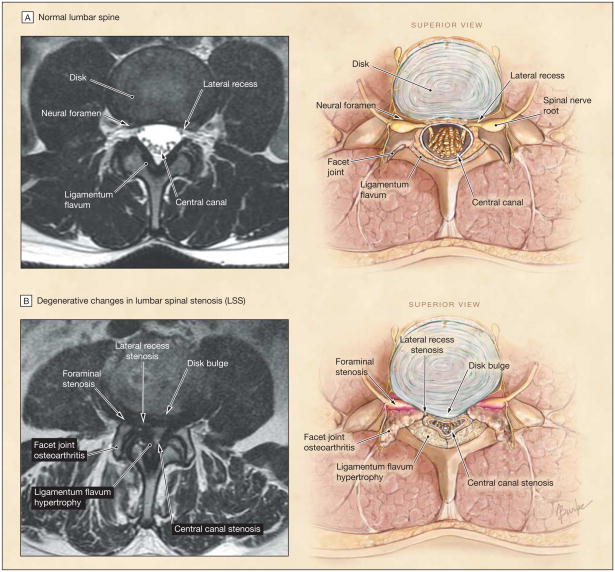
Context: The clinical syndrome of lumbar spinal stenosis (LSS) is a common diagnosis in older adults presenting with lower extremity pain.
Objective: To systematically review the accuracy of the clinical examination for the diagnosis of the clinical syndrome of LSS.
Data sources: MEDLINE, EMBASE, and CINAHL searches of articles published from January 1966 to September 2010.
Study selection: Studies were included if they contained adequate data on the accuracy of the history and physical examination for diagnosing the clinical syndrome of LSS, using a reference standard of expert opinion with radiographic or anatomic confirmation.
Data extraction: Two authors independently reviewed each study to determine eligibility, extract data, and appraise levels of evidence.
Data synthesis: Four studies evaluating 741 patients were identified. Among patients with lower extremity pain, the likelihood of the clinical syndrome of LSS was increased for individuals older than 70 years (likelihood ratio [LR], 2.0; 95% confidence interval [CI], 1.6-2.5), and was decreased for those younger than 60 years (LR, 0.40; 95% CI, 0.29-0.57). The most useful symptoms for increasing the likelihood of the clinical syndrome of LSS were having no pain when seated (LR, 7.4; 95% CI, 1.9-30), improvement of symptoms when bending forward (LR, 6.4; 95% CI, 4.1-9.9), the presence of bilateral buttock or leg pain (LR, 6.3; 95% CI, 3.1-13), and neurogenic claudication (LR, 3.7; 95% CI, 2.9-4.8). Absence of neurogenic claudication (LR, 0.23; 95% CI, 0.17-0.31) decreased the likelihood of the diagnosis. A wide-based gait (LR, 13; 95% CI, 1.9-95) and abnormal Romberg test result (LR, 4.2; 95% CI, 1.4-13) increased the likelihood of the clinical syndrome of LSS. A score of 7 or higher on a diagnostic support tool including history and examination findings increased the likelihood of the clinical syndrome of LSS (LR, 3.3; 95% CI, 2.7-4.0), while a score lower than 7 made the diagnosis much less likely (LR, 0.10; 95% CI, 0.06-0.16).
Conclusions: The diagnosis of the clinical syndrome of LSS requires the appropriate clinical picture and radiographic findings. Absence of pain when seated and improvement of symptoms when bending forward are the most useful individual findings. Combinations of findings are most useful for identifying patients who are unlikely to have the diagnosis.
Figures
References
-
- Vogt MT, Cawthon PM, Kang JD, Donaldson WF, Cauley JA, Nevitt MC. Prevalence of symptoms of cervical and lumbar stenosis among participants in the Osteoporotic Fractures in Men Study. Spine (Phila Pa 1976) 2006;31(13):1445–1451. - PubMed
-
- Hicks GE, Gaines JM, Shardell M, Simonsick EM. Associations of back and leg pain with health status and functional capacity of older adults: findings from the retirement community back pain study. Arthritis Rheum. 2008;59(9):1306–1313. - PubMed
-
- Katz JN, Harris MB. Clinical practice: lumbar spinal stenosis. N Engl J Med. 2008;358(8):818–825. - PubMed
-
- Fardon DF, Milette PC Combined Task Forces of the North American Spine Society, American Society of Spine Radiology, and American Society of Neuroradiology. Nomenclature and classification of lumbar disc pathology: recommendations of the Combined Task Forces of the North American Spine Society, American Society of Spine Radiology, and American Society of Neuroradiology. Spine (Phila Pa 1976) 2001;26(5):E93–E113. - PubMed
