

Defective glial maturation in vanishing white matter disease
- PMID: 21157376
- PMCID: PMC4135437
- DOI: 10.1097/NEN.0b013e318203ae74
Defective glial maturation in vanishing white matter disease
Abstract
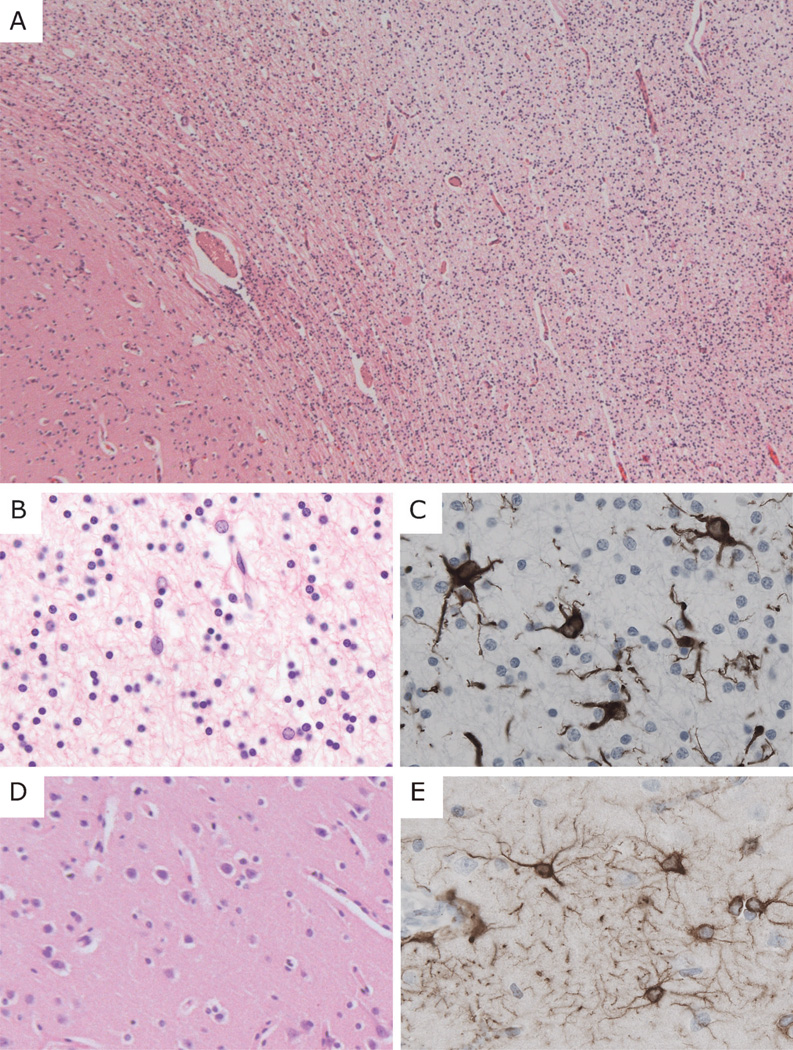
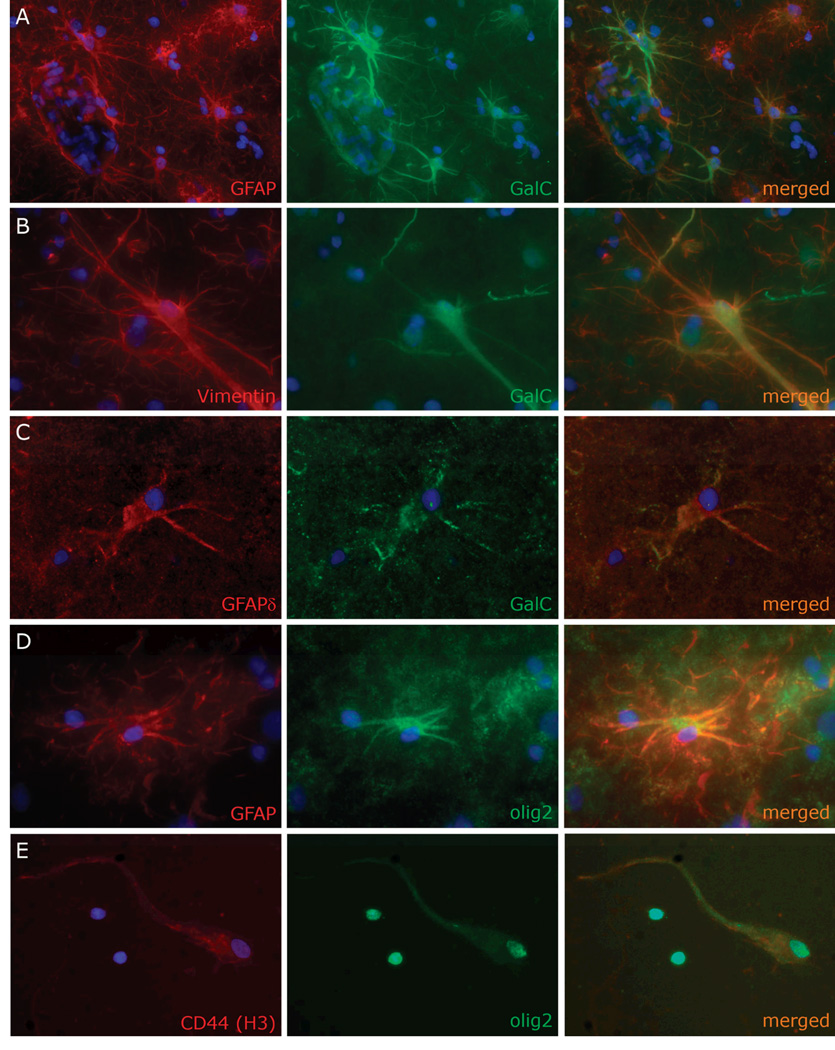
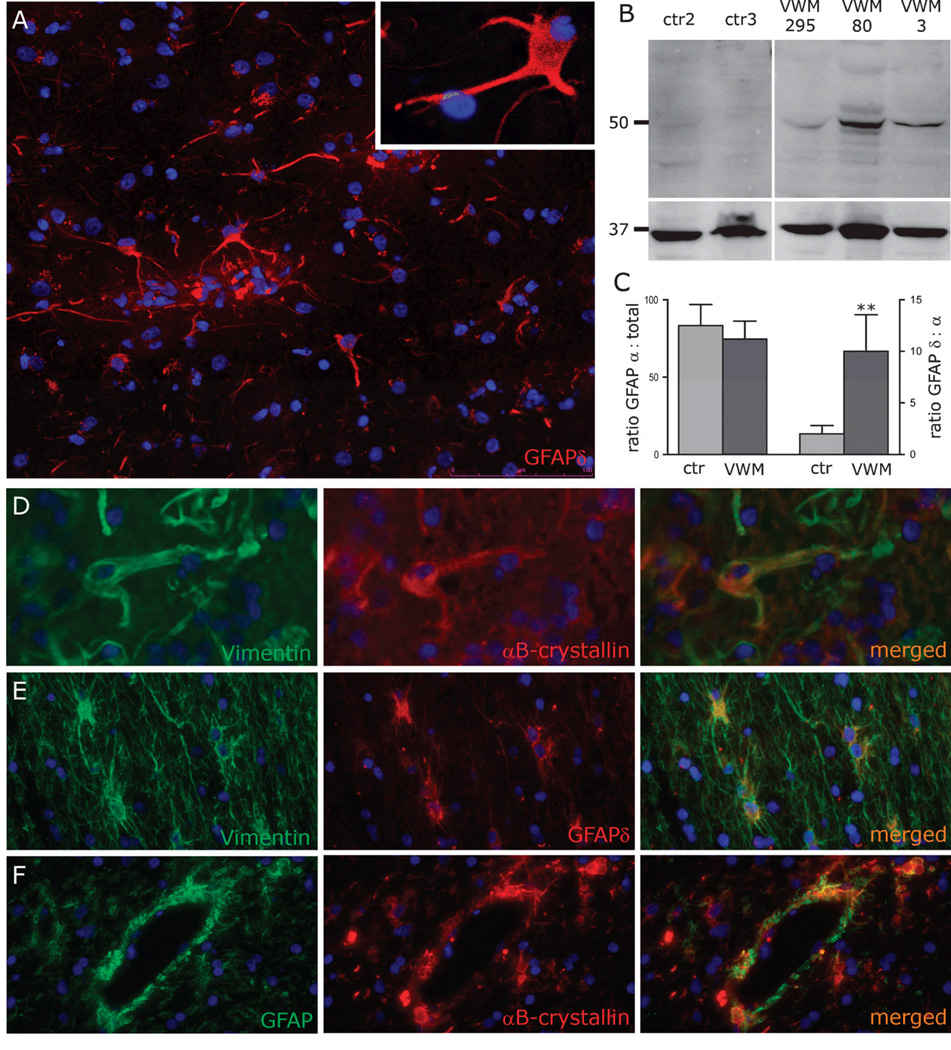
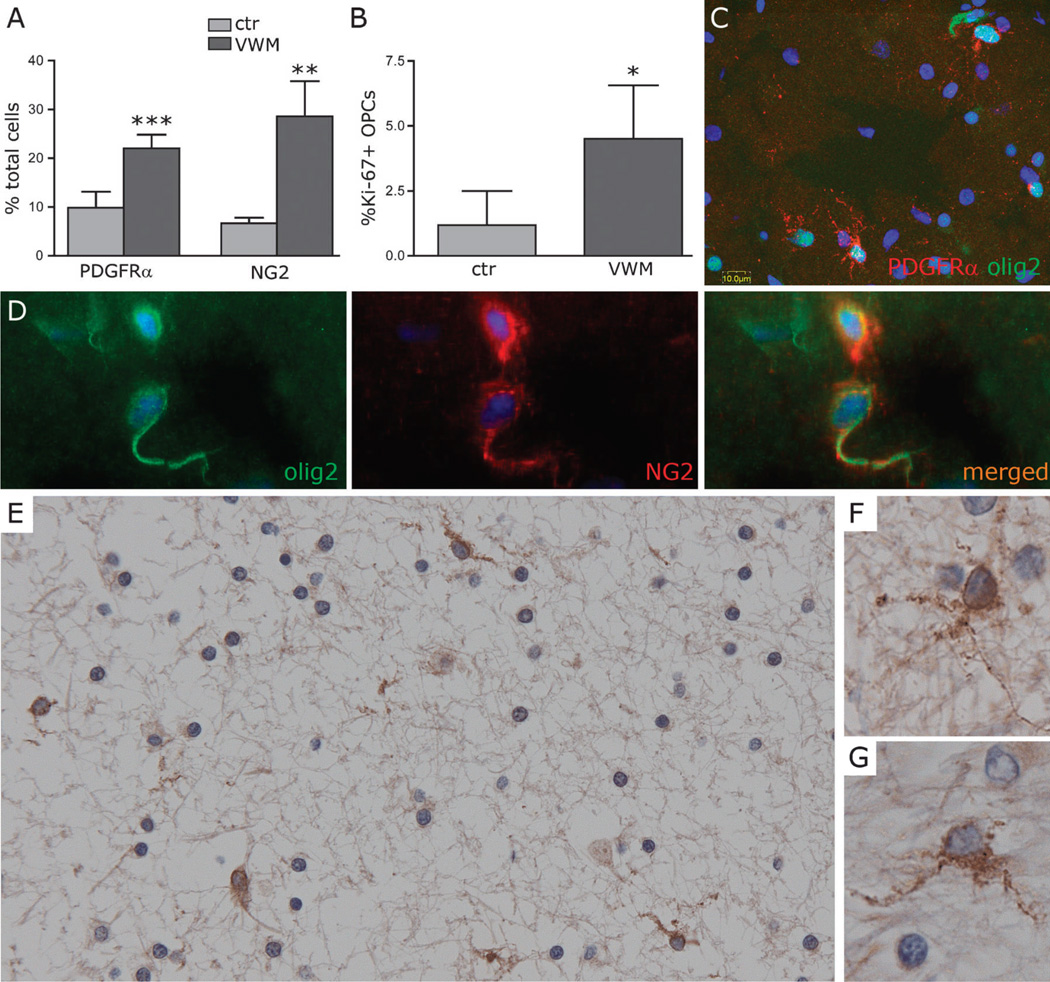
Vanishing white matter (VWM) disease is a genetic leukoencephalopathy linked to mutations in the eukaryotic translation initiation factor 2B. It is a disease of infants, children, and adults who experience a slowly progressive neurologic deterioration with episodes of rapid clinical worsening triggered by stress and eventually leading to death. Characteristic neuropathologic findings include cystic degeneration of the white matter with scarce reactive gliosis, dysmorphic astrocytes, and paucity of myelin despite an increase in oligodendrocytic density. To assess whether a defective maturation of macroglia may be responsible for the feeble gliosis and lack of myelin, weinvestigated the maturation status of astrocytes and oligodendrocytes in the brains of 8 VWM patients, 4 patients with other white matter disorders and 6 age-matched controls with a combination of immunocytochemistry, histochemistry, scratch-wound assays, Western blot, and quantitative polymerase chain reaction. We observed increased proliferation and a defect in the maturation of VWM astrocytes. They show an anomalous composition of their intermediate filament network with predominance of the δ-isoform of the glial fibrillary acidic protein and an increase in the heat shock protein αB-crystallin, supporting the possibility that a deficiency in astrocyte function may contribute to the loss of white matter in VWM. We also demonstrated a significant increase in numbers of premyelinating oligodendrocyte progenitors in VWM, which may explain the coexistence of oligodendrocytosis and myelin paucity in the patients' white matter.
Figures

References
-
- van der Knaap MS, Barth PG, Gabreels FJM, et al. A new leukoencephalopathy with vanishing white matter. Neurology. 1997;48:845–855. - PubMed
-
- Schiffmann R, Moller JR, Trapp BD, et al. Childhood ataxia with diffuse central nervous system hypomyelination. Ann Neurol. 1994;35:331–340. - PubMed
-
- Brück W, Herms J, Brockmann K, et al. Myelinopathia centralis diffusa (vanishing white matter disease): evidence of apoptotic oligodendrocyte degeneration in early lesion development. Ann Neurol. 2001;50:532–536. - PubMed
-
- van der Knaap MS, Pronk JC, Scheper GC. Vanishing white matter disease. Lancet Neurol. 2006;5:413–423. - PubMed
-
- Leegwater PA, Vermeulen G, Könst AA, et al. Subunits of the translation initiation factor eIF2B are mutant in leukoencephalopathy with vanishing white matter. Nat Genet. 2001;29:383–388. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
