

Thoracic target volume delineation using various maximum-intensity projection computed tomography image sets for radiotherapy treatment planning
- PMID: 21158293
- PMCID: PMC3810265
- DOI: 10.1118/1.3504605
Thoracic target volume delineation using various maximum-intensity projection computed tomography image sets for radiotherapy treatment planning
Abstract
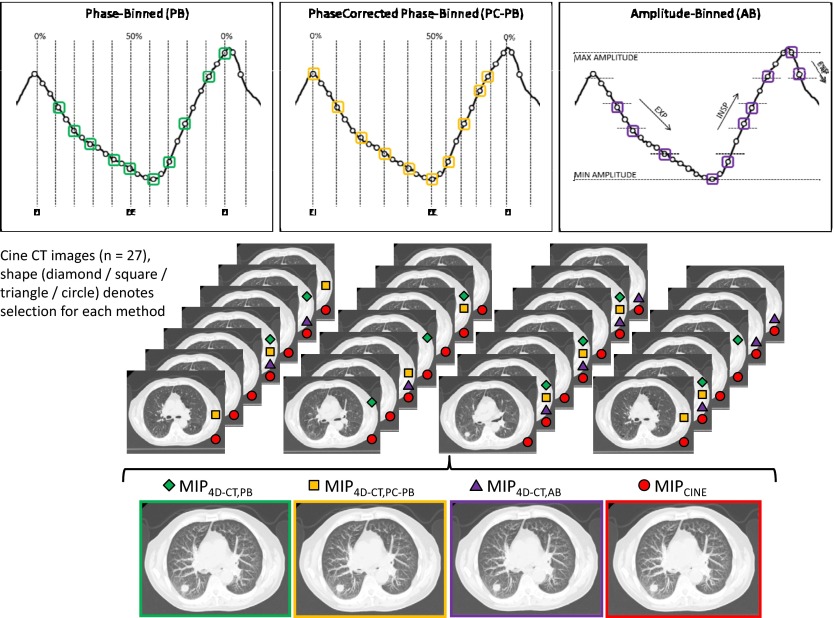
Purpose: Four-dimensional computed tomography (4D-CT) is commonly used to account for respiratory motion of target volumes in radiotherapy to the thorax. From the 4D-CT acquisition, a maximum-intensity projection (MIP) image set can be created and used to help define the tumor motion envelope or the internal gross tumor volume (iGTV). The purpose of this study was to quantify the differences in automatically contoured target volumes for usage in the delivery of stereotactic body radiation therapy using MIP data sets generated from one of the four methods: (1) 4D-CT phase-binned (PB) based on retrospective phase calculations, (2) 4D-CT phase-corrected phase-binned (PC-PB) based on motion extrema, (3) 4D-CT amplitude-binned (AB), and (4) cine CT built from all available images.
Methods: MIP image data sets using each of the four methods were generated for a cohort of 28 patients who had prior thoracic 4D-CT scans that exhibited lung tumor motion of at least 1 cm. Each MIP image set was automatically contoured on commercial radiation treatment planning system. Margins were added to the iGTV to observe differences in the final simulated planning target volumes (PTVs).
Results: For all patients, the iGTV measured on the MIP generated from the entire cine CT data set (iGTVcine) was the largest. Expressed as a percentage of iGTVcine, 4D-CT iGTV (all sorting methods) ranged from 83.8% to 99.1%, representing differences in the absolute volume ranging from 0.02 to 4.20 cm3; the largest average and range of 4D-CT iGTV measurements was from the PC-PB data set. Expressed as a percentage of PTVcine (expansions applied to iGTVeine), the 4D-CT PTV ranged from 87.6% to 99.6%, representing differences in the absolute volume ranging from 0.08 to 7.42 cm3. Regions of the measured respiratory waveform corresponding to a rapid change of phase or amplitude showed an increased susceptibility to the selection of identical images for adjacent bins. Duplicate image selection was most common in the AB implementation, followed by the PC-PB method. The authors also found that the image associated with the minimum amplitude measurement did not always correlate with the image that showed maximum tumor motion extent.
Conclusions: The authors identified cases in which the MIP generated from a 4D-CT sorting process under-represented the iGTV by more than 10% or up to 4.2 cm3 when compared to the iGTVcine. They suggest utilization of a MIP generated from the full cine CT data set to ensure maximum inclusive tumor extent.
Figures





References
-
- Mayo J. R., Muller N. L., and Henkelman R. M., “The double-fissure sign: A motion artifact on thin-section CT scans,” Radiology 165, 580–581 (1987). - PubMed
-
- Keall P. J., Mageras G. S., Balter J. M., Emery R. S., Forster K. M., Jiang S. B., Kapatoes J. M., Low D. A., Murphy M. J., Murray B. R., Ramsey C. R., Van Herk M. B., Vedam S. S., Wong J. W., and Yorke E., “The management of respiratory motion in radiation oncology report of AAPM Task Group 76,” Med. Phys. 33, 3874–3900 (2006). 10.1118/1.2349696 - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
