

An analytical review of vasculobiliary injury in laparoscopic and open cholecystectomy
- PMID: 21159098
- PMCID: PMC3019536
- DOI: 10.1111/j.1477-2574.2010.00225.x
An analytical review of vasculobiliary injury in laparoscopic and open cholecystectomy
Abstract
Objectives: Biliary injuries are frequently accompanied by vascular injuries, which may worsen the bile duct injury and cause liver ischemia. We performed an analytical review with the aim of defining vasculobiliary injury and setting out the important issues in this area.
Methods: A literature search of relevant terms was performed using OvidSP. Bibliographies of papers were also searched to obtain older literature.
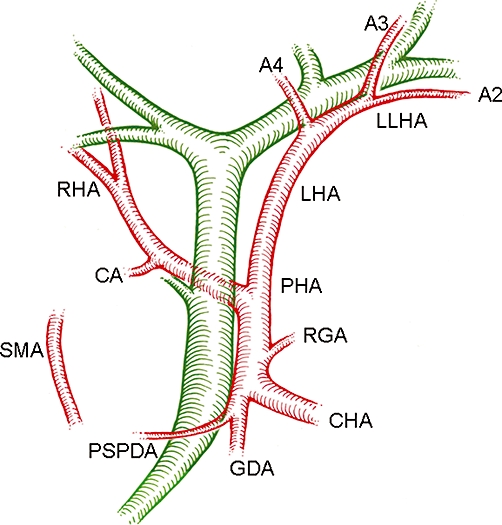
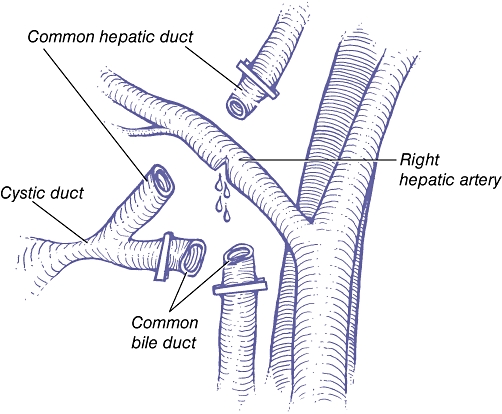
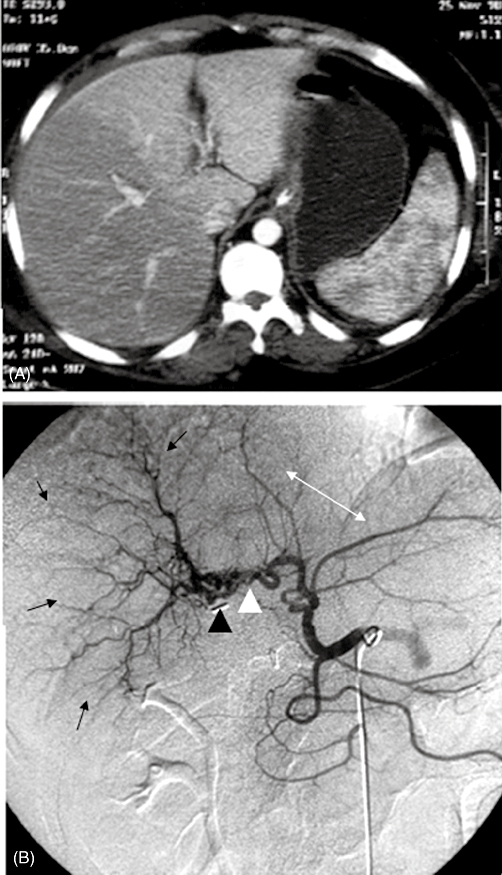
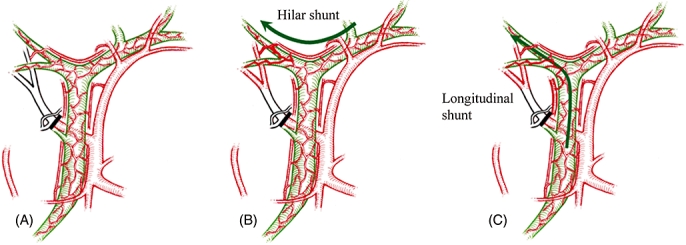
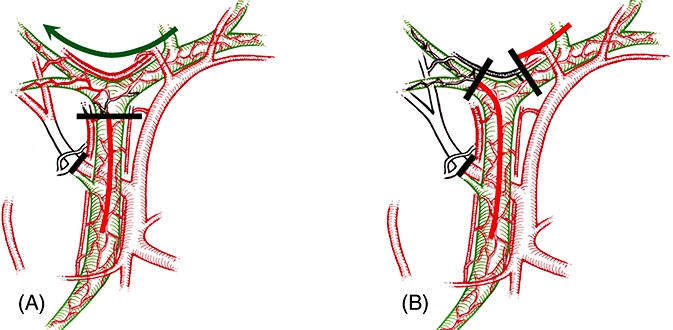
Results: Vasculobiliary injury was defined as: an injury to both a bile duct and a hepatic artery and/or portal vein; the bile duct injury may be caused by operative trauma, be ischaemic in origin or both, and may or may not be accompanied by various degrees of hepatic ischaemia. Right hepatic artery (RHA) vasculobiliary injury (VBI) is the most common variant. Injury to the RHA likely extends the biliary injury to a higher level than the gross observed mechanical injury. VBI results in slow hepatic infarction in about 10% of patients. Repair of the artery is rarely possible and the overall benefit unclear. Injuries involving the portal vein or common or proper hepatic arteries are much less common, but have more serious effects including rapid infarction of the liver.
Conclusions: Routine arteriography is recommended in patients with a biliary injury if early repair is contemplated. Consideration should be given to delaying repair of a biliary injury in patients with occlusion of the RHA. Patients with injuries to the portal vein or proper or common hepatic should be emergently referred to tertiary care centers.
© 2010 International Hepato-Pancreato-Biliary Association.
Figures
References
-
- Eisendrath DN. Operative injury of the common and hepatic bile ducts. Surg Gynecol Obstet. 1920;31:1–18.
-
- Anonymous. A prospective analysis of 1518 laparoscopic cholecystectomies. The Southern Surgeons Club. N Engl J Med. 1991;325:1517–1518. - PubMed
-
- Shapiro AL, Robillard GL. The arterial blood supply of the common and hepatic bile ducts with reference to the problems of common duct injury and repair; based on a series of 23 dissections. Surgery. 1948;23:1–11. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
