

Radiofrequency ablation of hepatocellular carcinoma as a bridge to liver transplantation
- PMID: 21159100
- PMCID: PMC3019538
- DOI: 10.1111/j.1477-2574.2010.00228.x
Radiofrequency ablation of hepatocellular carcinoma as a bridge to liver transplantation
Abstract
Background: Radiofrequency ablation (RFA) of hepatocellular carcinoma (HCC) is widely utilized as a bridge to liver transplant with limited evidence to support efficacy. The purpose of the present study was to measure the effect of RFA on time to drop-off in HCC-listed patients.
Methods: Patients with Milan criteria tumours listed between January 1999 and June 2007 were stratified into RFA (n= 77) and No Treatment groups (n= 93).
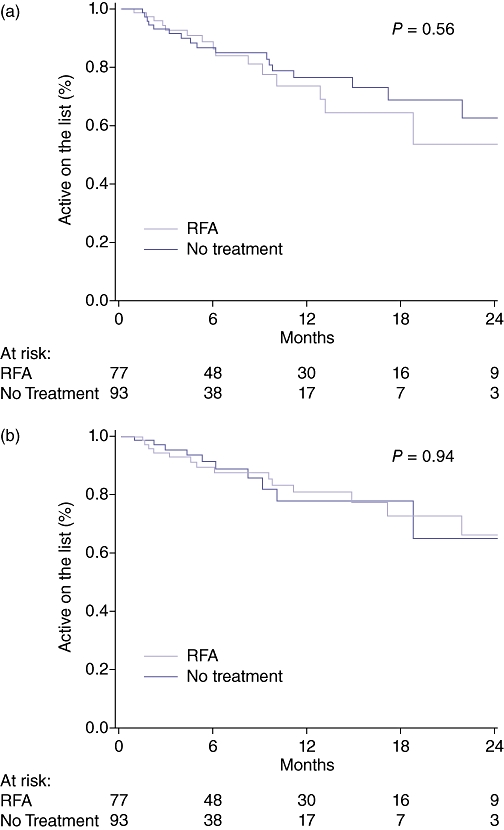
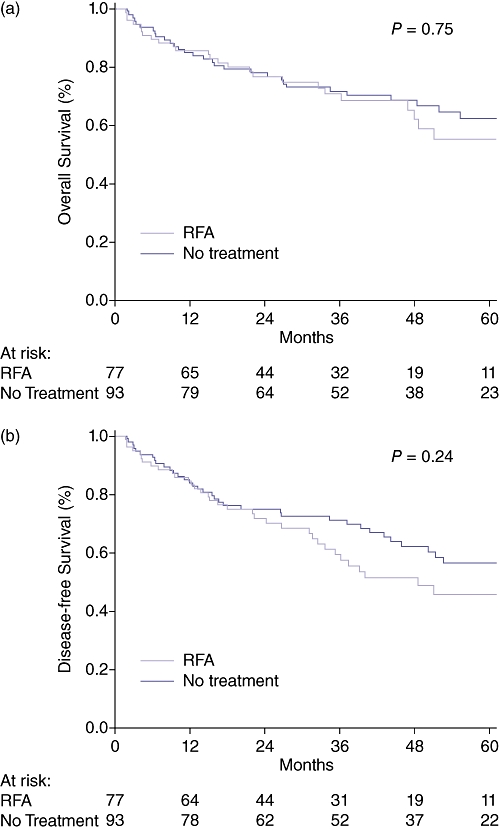
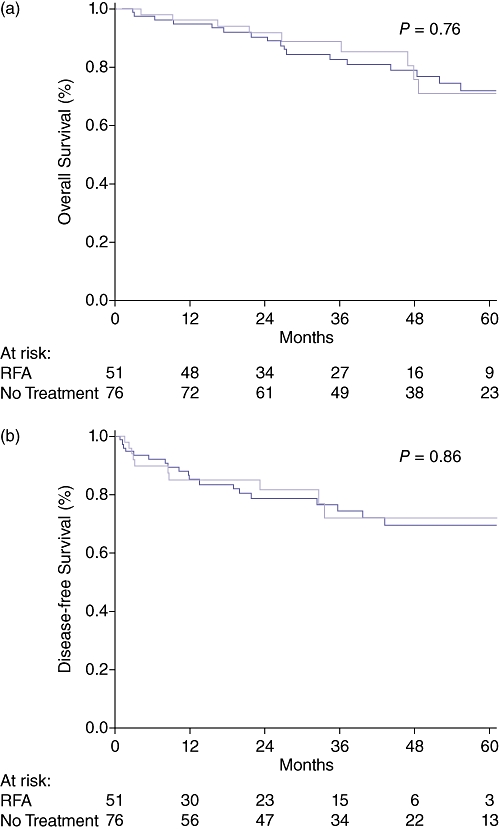
Results: The primary effectiveness of RFA was 83% (complete radiographic response). RFA was associated with a longer median wait time to transplant (9.5 vs. 5 months). Tumour-specific drop-off events were equivalent between RFA (21%) and No Treatment (12%) groups (P= 0.11). Controlling for wait time, there was no difference in overall (P= 0.56) or tumour-specific drop-off (P= 0.94). Furthermore, there were no differences in 5-year overall or tumour-free survivals from list date or transplant. Using multivariate analysis, the likelihood of receiving a transplant and patient survivals were associated with tumour characteristics (AFP, tumour number and size) and not with bridge therapy or waiting time.
Discussion: RFA allows patients to be maintained longer on the waiting list without negative consequences on drop-off or survival compared with no treatment. Post-transplant outcomes are affected more by tumour characteristics than RFA or wait time.
© 2010 International Hepato-Pancreato-Biliary Association.
Figures
References
-
- Mazzaferro V, Regalia E, Doci R, Andreola S, Pulvirenti A, Bozzetti F, et al. Liver transplantation for the treatment of small hepatocellular carcinomas in patients with cirrhosis. N Engl J Med. 1996;334:693–699. - PubMed
-
- Llovet JM, Fuster J, Bruix J. Intention-to-treat analysis of surgical treatment for early hepatocellular carcinoma: resection versus transplantation. Hepatology. 1999;30:1434–1440. - PubMed
-
- Shah SA, Cleary SP, Tan JC, Wei AC, Gallinger S, Grant DR, et al. An analysis of resection vs transplantation for early hepatocellular carcinoma: defining the optimal therapy at a single institution. Ann Surg Oncol. 2007;14:2608–2614. - PubMed
-
- Freeman RB, Edwards EB, Harper AM. Waiting list removal rates among patients with chronic and malignant liver diseases. Am J Transplant. 2006;6:1416–1421. - PubMed
-
- Di Bisceglie AM. Pretransplant treatments for hepatocellular carcinoma: do they improve outcomes? Liver Transpl. 2005;11(Suppl 2):S10–S13. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
