

Pancreatic head resectable adenocarcinoma: preoperative chemoradiation improves local control but does not affect survival
- PMID: 21159106
- PMCID: PMC3019544
- DOI: 10.1111/j.1477-2574.2010.00245.x
Pancreatic head resectable adenocarcinoma: preoperative chemoradiation improves local control but does not affect survival
Erratum in
- HPB (Oxford). 2011 Dec;13(12):899
Abstract
Background: This study assesses the impact of preoperative chemoradiation on recurrence, surgical morbidity, histopathological data and survival in resectable adenocarcinoma of the pancreatic head.
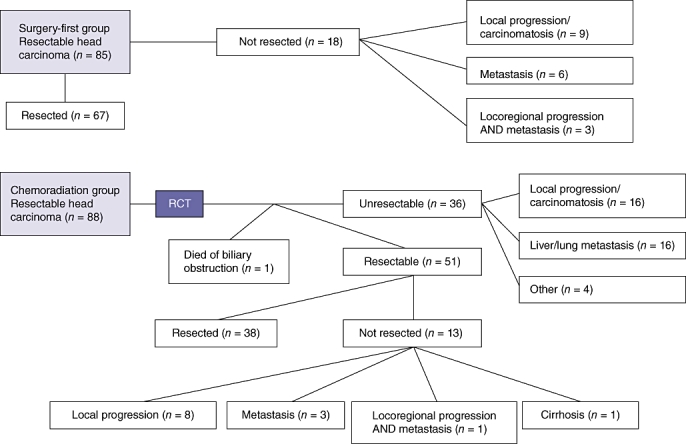
Methods: We carried out a retrospective study with an intention-to-treat analysis. From 1997 to 2006, 173 patients with resectable pancreas head carcinoma were treated in two reference centres in France using different treatment strategies.
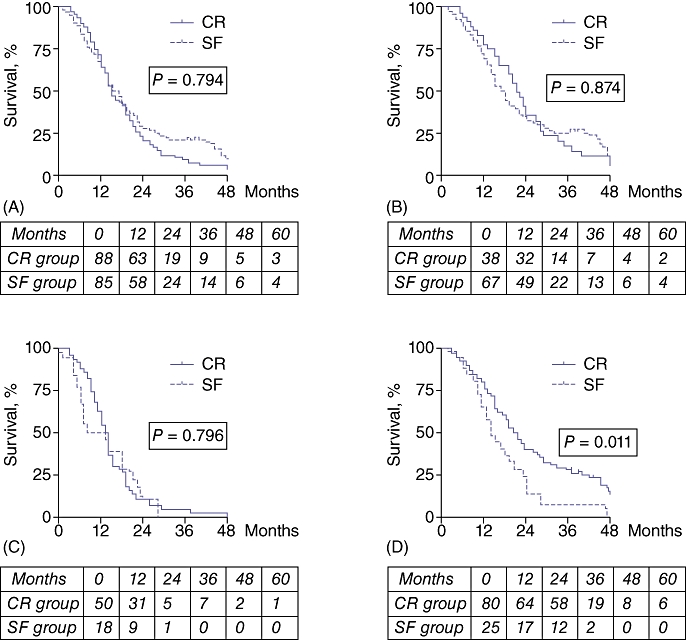
Results: Sixty-seven of 85 (79%) patients in the surgery-first (SF) group and 38 of 88 (43%) patients in the chemoradiation (CR) group underwent surgical resection (P < 0.001). Overall morbidity was 40% (15/38) in the CR group and 43% (29/67) in the SF group (P= 0.837). In the CR group, median tumour size was smaller (1.5 cm vs. 3.0 cm; P < 0.001) and fewer patients were node-positive (29% vs. 64%; P= 0.001) than in the SF group. There was less perineural (43% vs. 93%; P < 0.001), lymphatic and vascular (21% vs. 92%; P < 0.001) invasion in the CR group than in the SF group. In both groups, 89% of patients had recurrence (31/35 in the CR group and 57/64 in the SF group; P= 1.000), predominantly involving metastasis and carcinomatosis in the CR group (30/31 vs. 35/57; P < 0.001) and locoregional recurrence in the SF group (24/57 vs. 3/31; P= 0.002). Median survival for all patients and for resected patients in the CR and SF groups was, respectively, 15 months vs. 17 months, and 21 months vs. 18 months (P= non-significant).
Conclusions: Preoperative chemoradiation allows for good local control of the disease but does not increase survival, mainly for reasons of metastatic spread. Other options should be developed to improve both local and distant control of the disease.
© 2010 International Hepato-Pancreato-Biliary Association.
Figures
References
-
- National Cancer Institute, US National Institutes of Health. Pancreatic Cancer Treatment. 2010. http://www.cancer.gov. [Accessed 10 October 2010]
-
- Garcea G, Dennison AR, Pattenden CJ, Neal CP, Sutton CD, Berry DP. Survival following curative resection for pancreatic ductal adenocarcinoma. A systematic review of the literature. JOP. 2008;9:99–132. - PubMed
-
- Mancuso A, Calabro F, Sternberg CN. Current therapies and advances in the treatment of pancreatic cancer. Crit Rev Oncol Hematol. 2006;58:231–241. - PubMed
-
- Neoptolemos JP, Stocken DD, Friess H, Bassi C, Dunn JA, Hickey H, et al. European Study Group for Pancreatic Cancer A randomized trial of chemotherapy after resection of pancreatic cancer. New Egypt J Med. 2004;350:1200–1210. - PubMed
-
- Oettle H, Post S, Neuhaus P, Gellert K, Langrehr J, Ridwelski K, et al. Adjuvant chemotherapy with gemcitabine vs. observation in patients undergoing curative-intent resection of pancreatic cancer: a randomized controlled trial. JAMA. 2007;297:267–277. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
