

Case Reports
doi: 10.1186/2047-783x-15-11-504.
A fatal case of AIDS-defining meningoencephalitis by C. neoformans, sensitive to antifungal therapy
Affiliations
- PMID: 21159575
- PMCID: PMC3352659
- DOI: 10.1186/2047-783x-15-11-504
Item in Clipboard
Case Reports
A fatal case of AIDS-defining meningoencephalitis by C. neoformans, sensitive to antifungal therapy
Eur J Med Res.
.
Abstract
Cryptococcus neoformans is the most common cause of life threatening meningoencephalitis in HIV-infected patients. Diagnosis is based on tests for cryptoccocal antigen in serum and cerebrospinal fluid, and on culture of the organism. We present a case of AIDS-related cryptococcal meningoencephalitis unresponsive to antifungal combination therapy, despite of evidence of fungal susceptibility in vitro. Significant decreases in cryptococcal antigen titers in serum and cerebrospinal fluid did not correlate with progress in disease and fatal outcome.
Figures
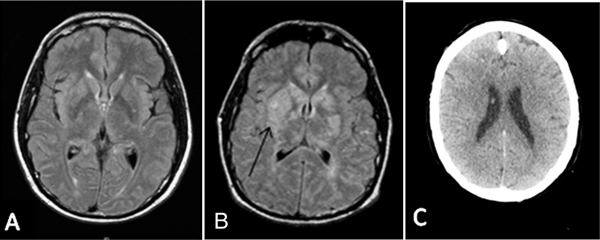
Series of cerebral images in the course of infection. A) cerebral MRI 3 weeks prior to admission; B) MRI on admission with bihemispheric mass right more than left in basal ganglia area (arrow); C) Cerebral CT after 3 weeks of antifungal combination therapy with loss of gray-white distinction and effacement of cerebral sulci.
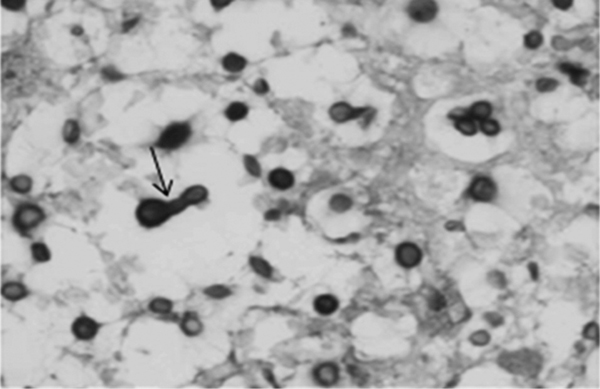
Brain tissue infection with encapsulated C. neoformans appears as bubbles due to gelatinous capsules. Reproducing by budding (arrow) PAS-stain, magnification, ×400.
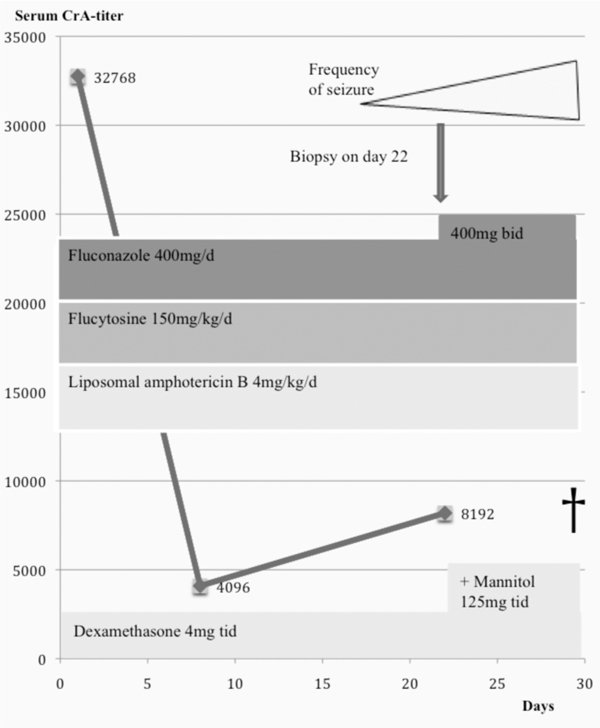
Course of serum cryptococal antigen titer, antifungal antigen titer, antifungal combination therapy, ICP controlling therapy and the course of disease.
Similar articles
-
Cryptoccocal meningitis in Yaoundé (Cameroon) HIV infected patients: Diagnosis, frequency and Cryptococcus neoformans isolates susceptibility study to fluconazole.J Mycol Med. 2015 Mar;25(1):11-6. doi: 10.1016/j.mycmed.2014.10.016. Epub 2014 Nov 21. J Mycol Med. 2015. PMID: 25467817
-
Clinical evaluation of the antifungal effect of sertraline in the treatment of cryptococcal meningitis in HIV patients: a single Mexican center experience.Infection. 2018 Feb;46(1):25-30. doi: 10.1007/s15010-017-1059-3. Epub 2017 Aug 16. Infection. 2018. PMID: 28815430 Clinical Trial.
-
Cryptococcal meningitis in AIDS.Indian J Med Sci. 2002 Dec;56(12):593-7. Indian J Med Sci. 2002. PMID: 14514241 Clinical Trial.
-
Cryptococcal meningitis due to Cryptococcus neoformans genotype AFLP1/VNI in Iran: a review of the literature.Mycoses. 2015 Dec;58(12):689-93. doi: 10.1111/myc.12415. Epub 2015 Oct 7. Mycoses. 2015. PMID: 26444438 Review.
-
Cryptococcal meningitis.Br J Hosp Med. 1995 Nov 1-14;54(9):439-45. Br J Hosp Med. 1995. PMID: 8564179 Review.
Cited by
-
Importance of follow-up cerebrospinal fluid analysis in cryptococcal meningoencephalitis.Dis Markers. 2014;2014:162576. doi: 10.1155/2014/162576. Epub 2014 Oct 13. Dis Markers. 2014. PMID: 25374433 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
