

Relationship between vitamin D, parathyroid hormone, and bone health
- PMID: 21159838
- PMCID: PMC3047227
- DOI: 10.1210/jc.2010-1886
Relationship between vitamin D, parathyroid hormone, and bone health
Abstract
Context: There is a controversy regarding the definition of vitamin D insufficiency as it relates to bone health.
Objective: The objective of the study was to examine the evidence for a threshold value of serum 25-hydroxyvitamin D (25OHD) that defines vitamin D insufficiency as it relates to bone health.
Design and participants: This was a cross-sectional analysis of baseline data in 488 elderly Caucasian women, mean age 71 yr, combined with a literature review of 70 studies on the relationship of serum PTH to serum 25OHD.
Setting: The study was conducted in independent-living women in the midwest United States.
Main outcome measure: The relationship between serum 25OHD, serum PTH, and serum osteocalcin and 24-h urine N-telopeptides was evaluated.
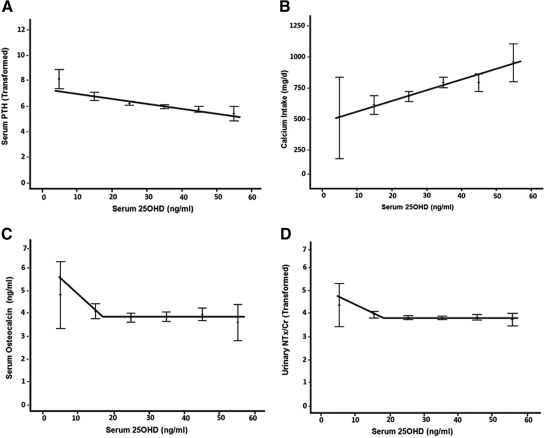
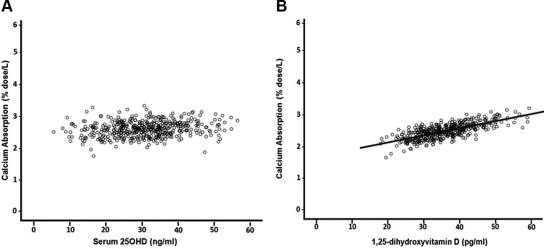
Results: Serum PTH was inversely correlated with serum 25OHD (r = -0.256, P < 0.0005), but no threshold as defined by suppression of serum PTH was found within the serum 25OHD range 6-60 ng/ml (15-150 nmol/liter). However, in contrast, there was a threshold for bone markers, serum osteocalcin and urine N-telopeptides, that increased only below a serum 25OHD of approximately 18 ng/ml (45 nmol/liter). Calcium absorption was not correlated with serum PTH and serum 25OHD, and no threshold was found. A literature review of 70 studies generally showed a threshold for serum PTH with increasing serum 25OHD, but there was no consistency in the threshold level of serum 25OHD that varied from 10 to 50 ng/ml (25-125 nmol/liter).
Conclusions: Vitamin D insufficiency should be defined as serum 25OHD less than 20 ng/ml (50 nmol/liter) as it relates to bone.
Figures

References
-
- World Health Organization Scientific Group on the Prevention and Management of Osteoporosis 2003. Prevention and management of osteoporosis: report of a WHO scientific group. Geneva: World Health Organization
-
- Dawson-Hughes B, Heaney RP, Holick MF, Lips P, Meunier PJ, Vieth R. 2005. Estimates of optimal vitamin D status. Osteoporos Int 16:713–716 - PubMed
-
- Holick MF. 2007. Vitamin D deficiency. N Engl J Med 357:266–281 - PubMed
-
- Ebeling PR, Sandgren ME, DiMagno EP, Lane AW, DeLuca HF, Riggs BL. 1992. Evidence of an age-related decrease in intestinal responsiveness to vitamin D: relationship between serum 1,25-dihydroxyvitamin D3 and intestinal vitamin D receptor concentrations in normal women. J Clin Endocrinol Metab 75:176–182 - PubMed
-
- Gannagé-Yared MH, Chemali R, Yaacoub N, Halaby G. 2000. Hypovitaminosis D in a sunny country: relation to lifestyle and bone markers. J Bone Miner Res 15:1856–1862 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
