

The current status of cone beam computed tomography imaging in orthodontics
- PMID: 21159912
- PMCID: PMC3611465
- DOI: 10.1259/dmfr/12615645
The current status of cone beam computed tomography imaging in orthodontics
Abstract
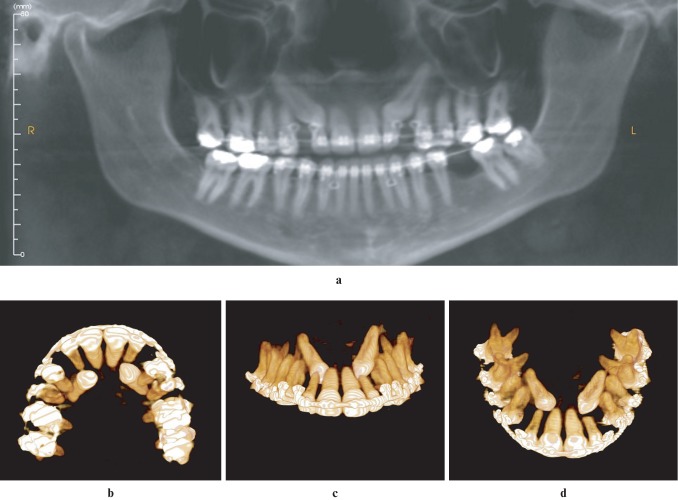
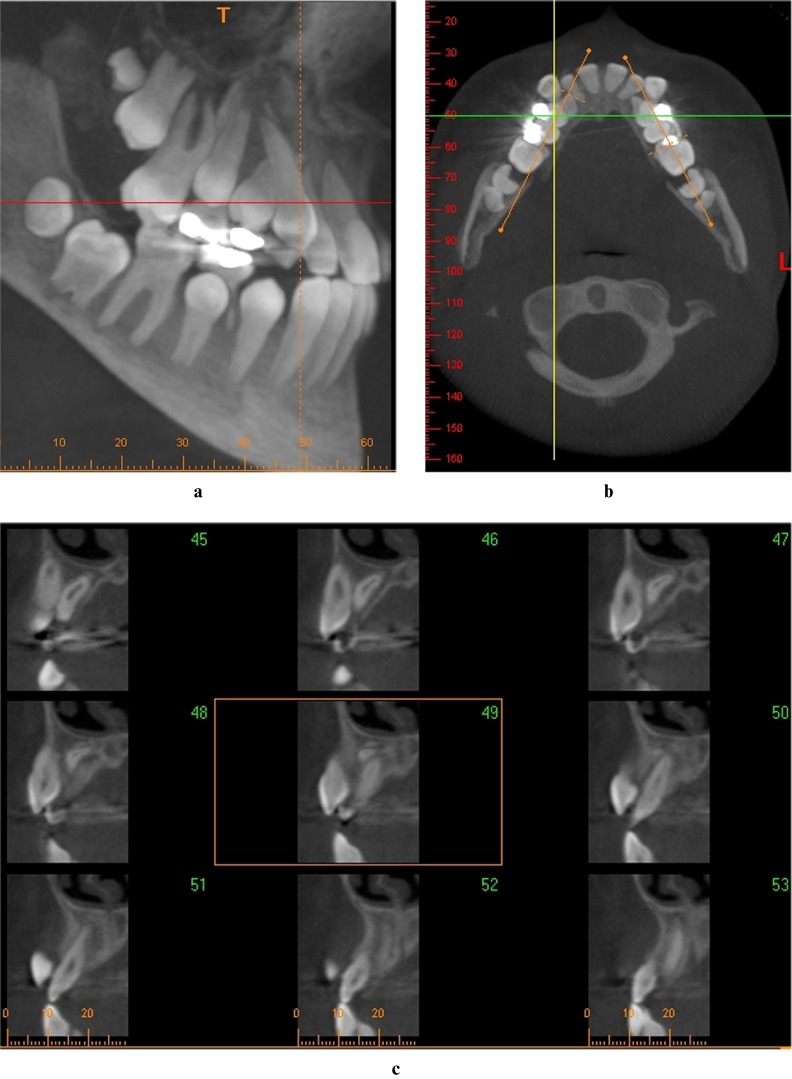
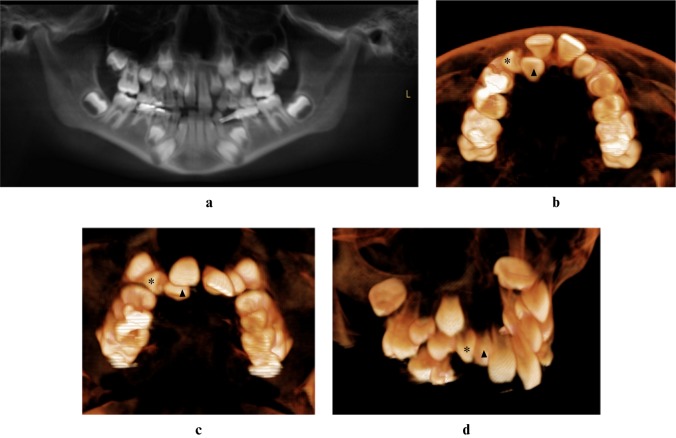
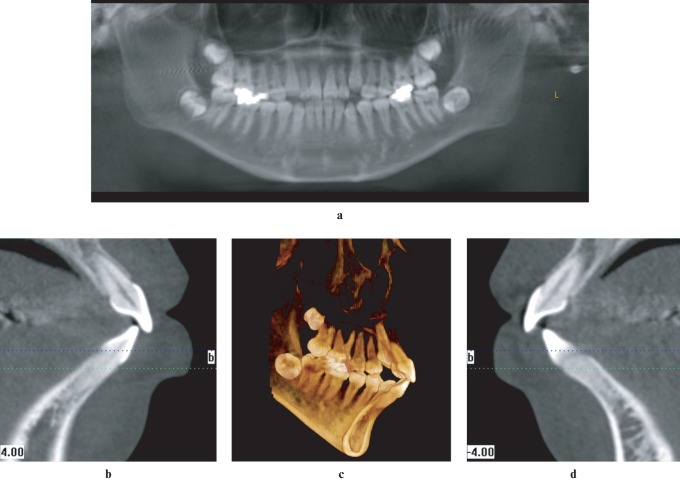
Cone beam CT (CBCT) has become an increasingly important source of three dimensional (3D) volumetric data in clinical orthodontics since its introduction into dentistry in 1998. The purpose of this manuscript is to highlight the current understanding of, and evidence for, the clinical use of CBCT in orthodontics, and to review the findings to answer clinically relevant questions. Currently available information from studies using CBCT can be organized into five broad categories: 1, the assessment of CBCT technology; 2, its use in craniofacial morphometric analyses; 3, incidental and missed findings; 4, analysis of treatment outcomes; and 5, efficacy of CBCT in diagnosis and treatment planning. The findings in these topical areas are summarized, followed by current indications and protocols for the use of CBCT in specific cases. Despite the increasing popularity of CBCT in orthodontics, and its advantages over routine radiography in specific cases, the effects of information derived from these images in altering diagnosis and treatment decisions has not been demonstrated in several types of cases. It has therefore been recommended that CBCT be used in select cases in which conventional radiography cannot supply satisfactory diagnostic information; these include cleft palate patients, assessment of unerupted tooth position, supernumerary teeth, identification of root resorption and for planning orthognathic surgery. The need to image other types of cases should be made on a case-by-case basis following an assessment of benefits vs risks of scanning in these situations.
Figures

References
-
- Shortliffe E, Perreault LE, Wiederhold G, Fagan LM. Medical informatics: computer applications in health care and biomedicine. 2nd edn. New York: Springer;2001
-
- Tsao DH, Kazanoglu A, McCasland JP. Measurability of radiographic images. Am J Orthod 1983;84:212–216 - PubMed
-
- Adams GL, Gansky SA, Miller AJ, Harrell WE, Jr, Hatcher DC. Comparison between traditional 2-dimensional cephalometry and a 3-dimensional approach on human dry skulls. Am J Orthod Dentofacial Orthop 2004;126:397–409 - PubMed
-
- Harrell WE., Jr 3D Diagnosis and treatment planning in orthodontics. Semin in Orthod 2009;15:35–41
-
- Harrell WE, Jr, Hatcher DC, Bolt RL. In search of anatomic truth: 3-dimensional digital modeling and the future of orthodontics. Am J Orthod Dentofacial Orthop 2002;122:325–330 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
