

doi: 10.4240/wjgs.v2.i10.331.
Differentiating intraductal papillary mucinous neoplasms from other pancreatic cystic lesions
Affiliations
- PMID: 21160839
- PMCID: PMC2999201
- DOI: 10.4240/wjgs.v2.i10.331
Item in Clipboard
Differentiating intraductal papillary mucinous neoplasms from other pancreatic cystic lesions
World J Gastrointest Surg.
.
Abstract
Intraductal papillary mucinous neoplasms (IPMN) can be difficult to distinguish from other cystic lesions of the pancreas. To understand better and discuss the current knowledge on this topic, the literature and the institutional experience at a large pancreatic disease center have been reviewed. A combination of preoperative demographic, historical, radiographic, laboratory data, as well as postoperative pathologic analyses can often distinguish IPMN from other lesions in the differential diagnosis.
Keywords: Differential diagnosis; Intraductal papillary mucinous neoplasms; Pancreas cancer; Pancreatic cyst.
Figures
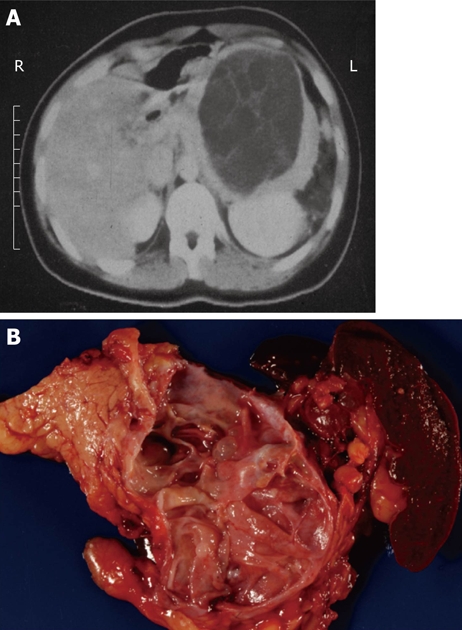
Typical computed tomography (A) and gross (B) appearance of a mucinous cystic neoplasm showing the distal location and the lack of communication with the duct, respectively.

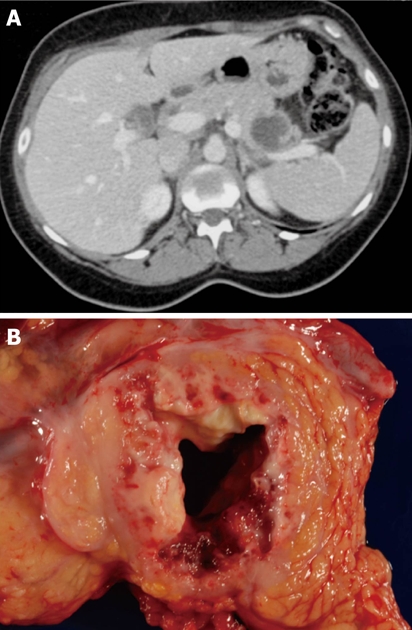
Typical computed tomography (A) and gross (B) appearance of a small pancreatic pseudocyst showing the typical spheroid shape, unilocularity, and necrotic debris contents.
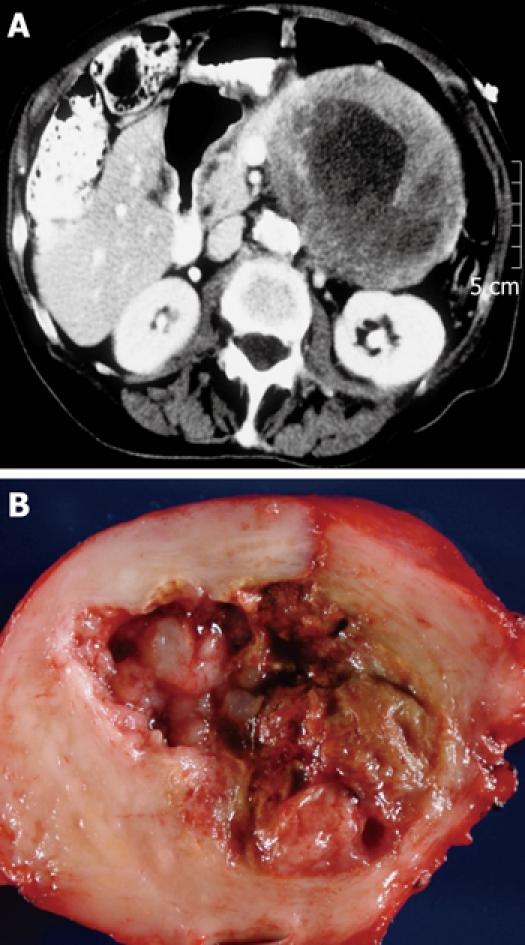
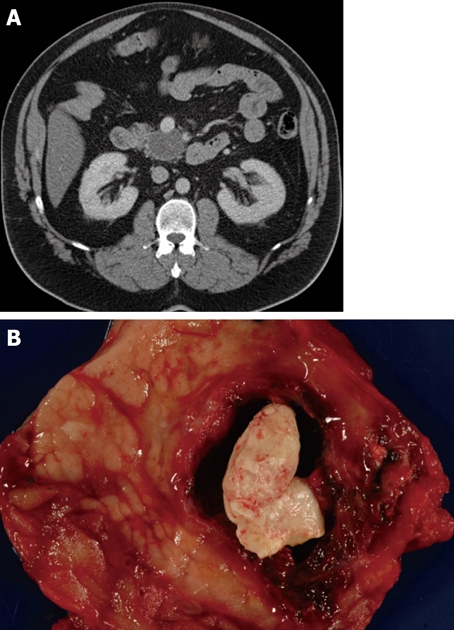
Typical computed tomography (A) and gross (B) appearance of a solid pseudopapillary neoplasm showing the typical ovoid shape and necrotic debris contents.
Typical computed tomography (A) and gross (B) appearance of a serous cystadenoma showing the honeycomb appearance.
Typical computed tomography (A) and gross (B) appearance of a cystic neuroendocrine tumor showing the spherical shape and the occasionally seen calcification.
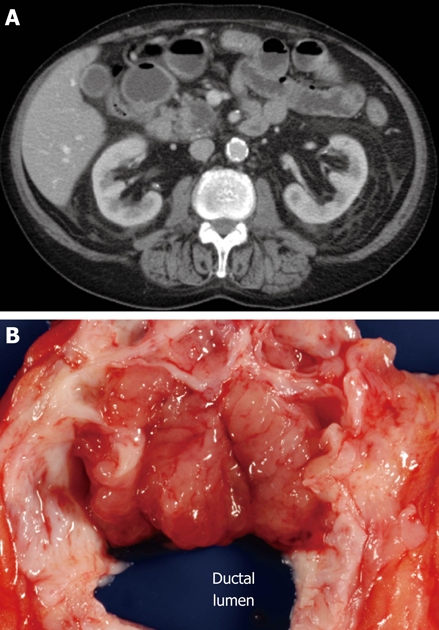
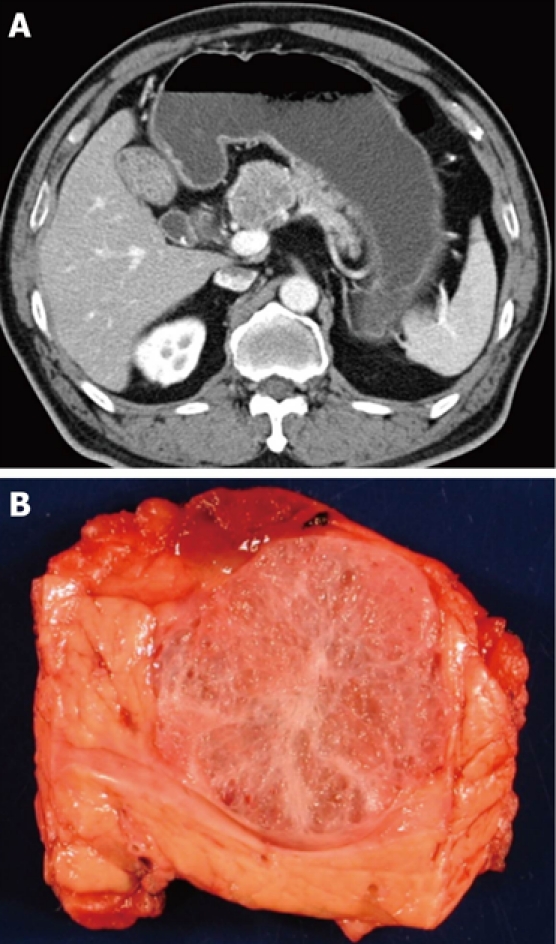
Typical computed tomography (A) and gross (B) appearance of an intraductal papillary mucinous neoplasm showing the ovoid shape and communication with the duct, respectively.
Typical computed tomography (A) and gross (B) appearance of a lymphoepithelial cyst showing the typical ovoid shape, peripheral location, and proteinaceous concretions (not always present on computed tomography imaging).
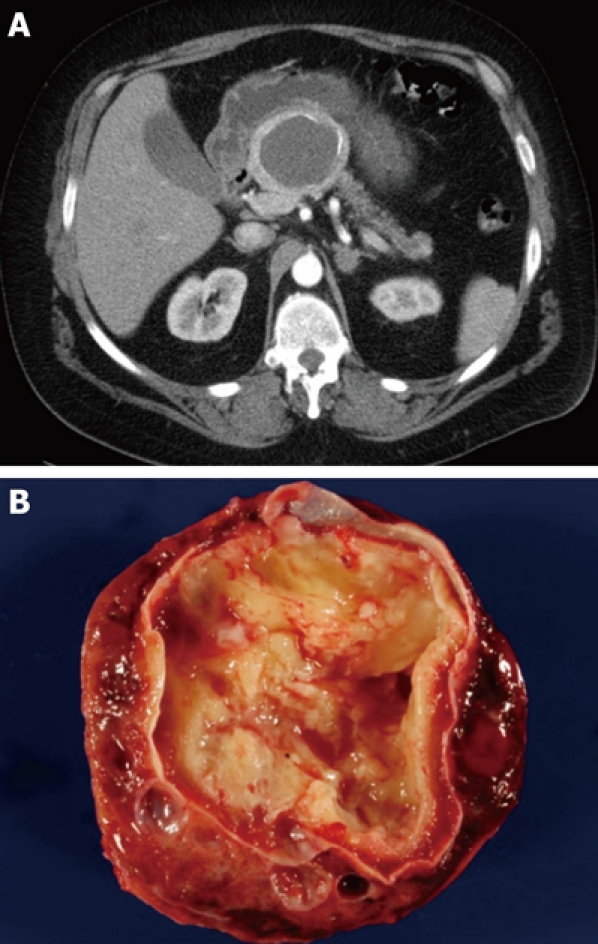
Typical computed tomography (A) and gross (B) appearance of an invasive carcinoma with cystic degeneration.
Similar articles
-
Intraductal oncocytic papillary neoplasm of the pancreas: a case of a second neoplasm in a pancreas cancer survivor.JOP. 2015 Jan 31;16(1):63-5. doi: 10.6092/1590-8577/2899. JOP. 2015. PMID: 25640786
-
Systematic review of the utility of 18-FDG PET in the preoperative evaluation of IPMNs and cystic lesions of the pancreas.Surgery. 2019 May;165(5):929-937. doi: 10.1016/j.surg.2018.11.006. Epub 2018 Dec 18. Surgery. 2019. PMID: 30577952
-
Mucin-producing neoplasms of the pancreas. Intraductal papillary and mucinous cystic neoplasms.Ann Surg. 1996 Feb;223(2):141-6. doi: 10.1097/00000658-199602000-00005. Ann Surg. 1996. PMID: 8597507 Free PMC article. Review.
-
[Intraductal papillary mucinous neoplasm of the pancreas (IPMN)--standards and new aspects].Zentralbl Chir. 2014 Jun;139(3):308-17. doi: 10.1055/s-0033-1350892. Epub 2013 Nov 15. Zentralbl Chir. 2014. PMID: 24241954 Review. German.
-
Clinicopathologic characteristics of patients with resected multifocal intraductal papillary mucinous neoplasm of the pancreas.Surgery. 2012 Sep;152(3 Suppl 1):S74-80. doi: 10.1016/j.surg.2012.05.025. Epub 2012 Jul 6. Surgery. 2012. PMID: 22770954
Cited by
-
Colloid Carcinoma of the Pancreas with a Series of Radiological and Pathological Studies for Diagnosis: A Case Report.Diagnostics (Basel). 2022 Jan 22;12(2):282. doi: 10.3390/diagnostics12020282. Diagnostics (Basel). 2022. PMID: 35204372 Free PMC article.
-
A mixed-type intraductal papillary mucinous neoplasm of the pancreas with a histologic combination of gastric and pancreatobiliary subtypes in a 70-year-old woman: a case report.J Med Case Rep. 2020 Sep 9;14(1):146. doi: 10.1186/s13256-020-02464-z. J Med Case Rep. 2020. PMID: 32900376 Free PMC article.
-
Diagnosis and management of cystic lesions of the pancreas.Diagn Ther Endosc. 2011;2011:478913. doi: 10.1155/2011/478913. Epub 2011 Aug 22. Diagn Ther Endosc. 2011. PMID: 21904442 Free PMC article.
-
Comparison of surgical and endoscopic sample collection for pancreatic cyst fluid biomarker identification.J Proteome Res. 2012 May 4;11(5):2904-11. doi: 10.1021/pr2012736. Epub 2012 Apr 4. J Proteome Res. 2012. PMID: 22439797 Free PMC article.
-
[Pathology and classification of intraductal papillary mucinous neoplasms of the pancreas].Chirurg. 2012 Feb;83(2):110-5. doi: 10.1007/s00104-011-2181-x. Chirurg. 2012. PMID: 22271052 Review. German.
References
-
- Klöppel G, Heitz PU, Capella C, Solcia E. Pathology and nomenclature of human gastrointestinal neuroendocrine (carcinoid) tumors and related lesions. World J Surg. 1996;20:132–141. - PubMed
-
- Hruban RH, Pitman MB, Klimstra DS. Tumors of the Pancreas. Washington, DC: American Registry of Pathology; 2007.
-
- Crippa S, Fernández-Del Castillo C, Salvia R, Finkelstein D, Bassi C, Domínguez I, Muzikansky A, Thayer SP, Falconi M, Mino-Kenudson M, et al. Mucin-producing neoplasms of the pancreas: an analysis of distinguishing clinical and epidemiologic characteristics. Clin Gastroenterol Hepatol. 2010;8:213–219. - PMC - PubMed
LinkOut - more resources
Full Text Sources
