

Multidisciplinary therapy for treatment of patients with peritoneal carcinomatosis from gastric cancer
- PMID: 21160926
- PMCID: PMC2998933
- DOI: 10.4251/wjgo.v2.i2.85
Multidisciplinary therapy for treatment of patients with peritoneal carcinomatosis from gastric cancer
Abstract
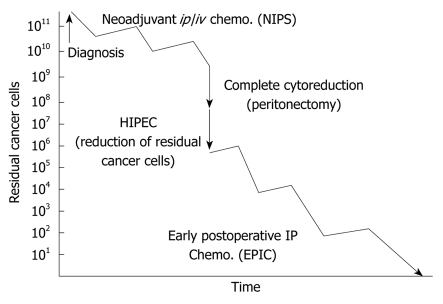
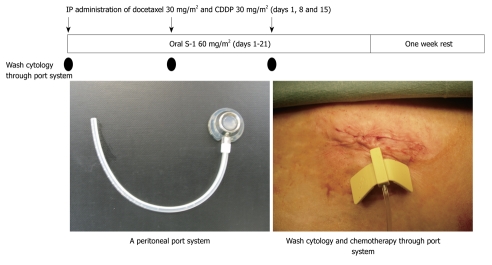
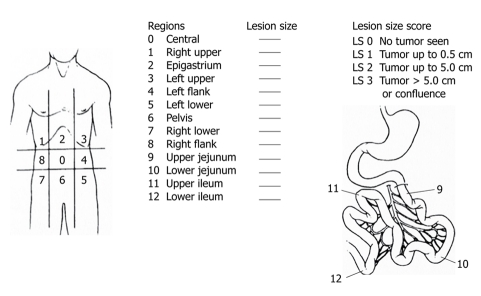
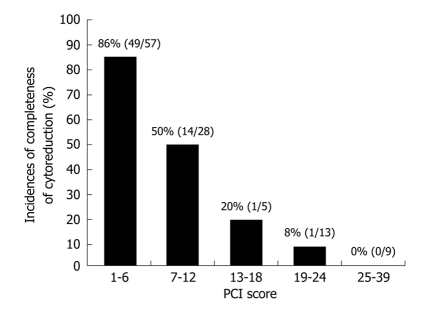
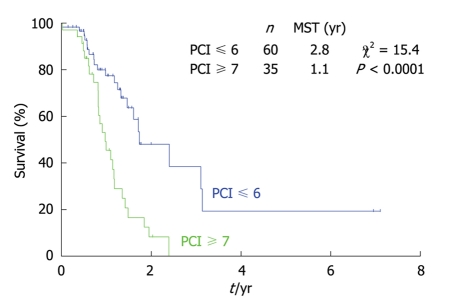
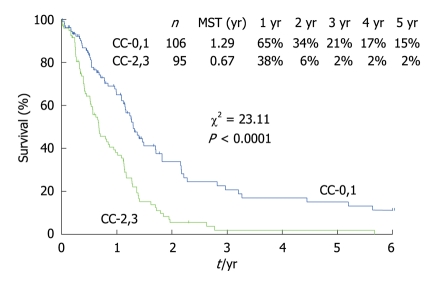
There is no standard treatment for peritoneal carcinomatosis (PC) from gastric cancer. A novel multidisciplinary treatment combining bidirectional chemotherapy [neoadjuvant intraperitoneal-systemic chemotherapy protocol (NIPS)], peritonectomy, hyperthermic intraperitoneal chemoperfusion (HIPEC) and early postoperative intraperitoneal chemotherapy has been developed. In this article, we assess the indications, safety and efficacy of this treatment, review the relevant studies and introduce our experiences. The aims of NIPS are stage reduction, the eradication of peritoneal free cancer cells, and an increased incidence of complete cytoreduction (CC-0) for PC. A complete response after NIPS was obtained in 15 (50%) out of 30 patients with PC. Thus, a significantly high incidence of CC-0 can be obtained in patients with a peritoneal cancer index (PCI) ≤ 6. Using a multivariate analysis to examine the survival benefit, CC-0 and NIPS are identified as significant indicators of a good outcome. However, the high morbidity and mortality rates associated with peritonectomy and perioperative chemotherapy make stringent patient selection important. The best indications for multidisciplinary therapy are localized PC (PCI ≤ 6) from resectable gastric cancer that can be completely removed during a peritonectomy. NIPS and complete cytoreduction are essential treatment modalities for improving the survival of patients with PC from gastric cancer.
Keywords: Chemotherapy; Gastric cancer; Peritoneal carcinomatosis.
Figures
References
-
- Yonemura Y, Kawamura T, Bandou E, Tsukiyama G, Endou Y, Miura M. The natural history of free cancer cells in the peritoneal cavity. In: Gonzalez-Moreno S, editor. Advances in peritoneal surface oncology. Berlin: Springer; 2007. pp. 11–23. - PubMed
-
- Chu DZ, Lang NP, Thompson C, Osteen PK, Westbrook KC. Peritoneal carcinomatosis in nongynecologic malignancy. A prospective study of prognostic factors. Cancer. 1989;63:364–367. - PubMed
-
- Sugarbaker PH, Yonemura Y. Clinical pathway for the management of resectable gastric cancer with peritoneal seeding: best palliation with a ray of hope for cure. Oncology. 2000;58:96–107. - PubMed
-
- Yonemura Y, Bandou E, Kinoshita K, Kawamura T, Takahashi S, Endou Y, Sasaki T. Effective therapy for peritoneal dissemination in gastric cancer. Surg Oncol Clin N Am. 2003;12:635–648. - PubMed
-
- MacDonald JS, Schein PS, Woolley PV, Smythe T, Ueno W, Hoth D, Smith F, Boiron M, Gisselbrecht C, Brunet R, et al. 5-Fluorouracil, doxorubicin, and mitomycin (FAM) combination chemotherapy for advanced gastric cancer. Ann Intern Med. 1980;93:533–536. - PubMed
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
