

Synchronous development of HCC and CCC in the same subsegment of the liver in a patient with type C liver cirrhosis
- PMID: 21160972
- PMCID: PMC2998951
- DOI: 10.4254/wjh.v1.i1.103
Synchronous development of HCC and CCC in the same subsegment of the liver in a patient with type C liver cirrhosis
Abstract
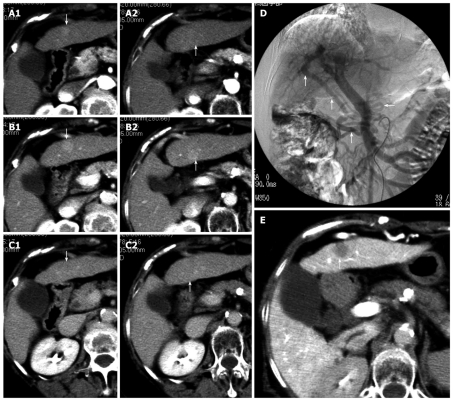
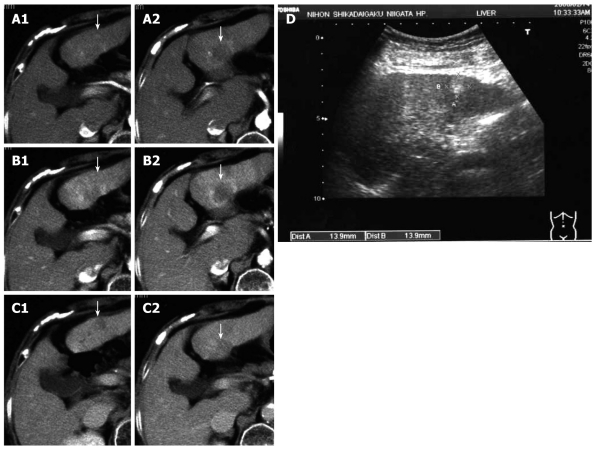
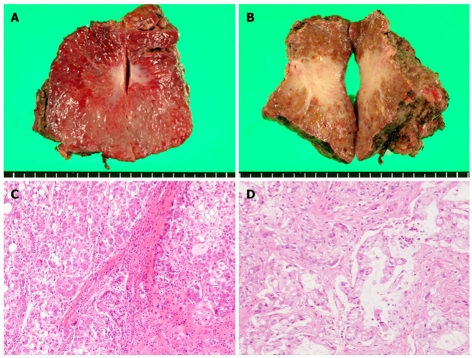
As a result of having undergone computed tomography (CT), a 75-year-old woman with type-C liver cirrhosiswas shown to have two tumors on the ventral and dorsal sides of subsegment 3 (S3). The tumor on the ventral side was diagnosed as a classic hepatocellular carcinoma (HCC), while that on the dorsal side was considered atypical for a HCC. Although the indocyanine green (ICG) findings indicated poor hepatic reserve, the prothrombin time (PT) was relatively good. An operation was performed in February 2007; however, this resulted in exploratory laparotomy. Dynamic CT performed 12 mo after the operation revealed that the tumor on the dorsal side of S3 had apparently increased. The marginal portion of the tumor was shown to be in the early and parenchymal phases, while the internal portion was found to have grown only slightly in the delayed phase. We diagnosed this tumor as a cholangiocellular carcinoma (CCC). S3 subsegmentectomy was performed in April 2008. The tumor on the ventral side was pathologically diagnosed as a moderately differentiated HCC, and that on the dorsal side was diagnosed as a CCC. We can therefore report a rare case of synchronous development of HCC and CCC in the same subsegment of the liver in a patient with type-C liver cirrhosis. We also add a literature review for all the reported cases published in Japan and around the world, and summarize the features of double cancer exhibiting both HCC and CCC.
Keywords: Cholangiocellular carcinoma; Double cancer; Hepatocellular carcinoma; Literature review; Synchronous.
Figures
References
-
- Yamaoka Y, Ikai I, Sakai Y, Okita K, Omata M, Kojiro M, Kobayashi K, Nakanuma Y, Nikawa T, Makuuchi M. Report of the 15th nationwide follow-up survey of primary liver cancer in Japan (In Japanese) Kanzo. 2003;44:157–175.
-
- Ikai I, Arii S, Ichida T, Okita K, Omata M, Kojiro M, Takayasu K, Nakanuma Y, Makuuchi M, Matsuyama Y, et al. Report of the 16th follow-up survey of primary liver cancer. Hepatol Res. 2005;32:163–172. - PubMed
-
- Ikai I, Arii S, Okazaki M, Okita K, Omata M, Kojiro M, Takayasu K, Nakanuma Y, Makuuchi M, Matsuyama Y, et al. Report of the 17th Nationwide Follow-up Survey of Primary Liver Cancer in Japan. Hepatol Res. 2007;37:676–691. - PubMed
-
- Mitsui T, Makuuchi M, Kurohiji T. [Resected case of primary liver cancer with separate two tumors of hepatocellular carcinoma and cholangiocellular carcinoma.] Kanzo. 1986;27:64–69.
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
