

Prognosis of metastatic splenic hilum lymph node in patients with gastric cancer after total gastrectomy and splenectomy
- PMID: 21160977
- PMCID: PMC2998958
- DOI: 10.4254/wjh.v2.i2.81
Prognosis of metastatic splenic hilum lymph node in patients with gastric cancer after total gastrectomy and splenectomy
Abstract
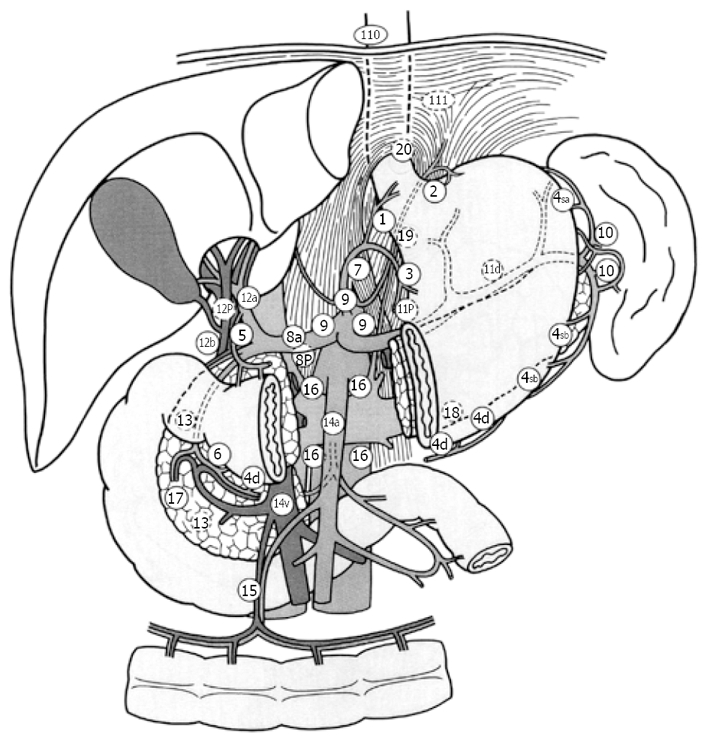
Aim: To clarify the significance of combined resection of the spleen to dissect the No. 10 lymph node (LN).
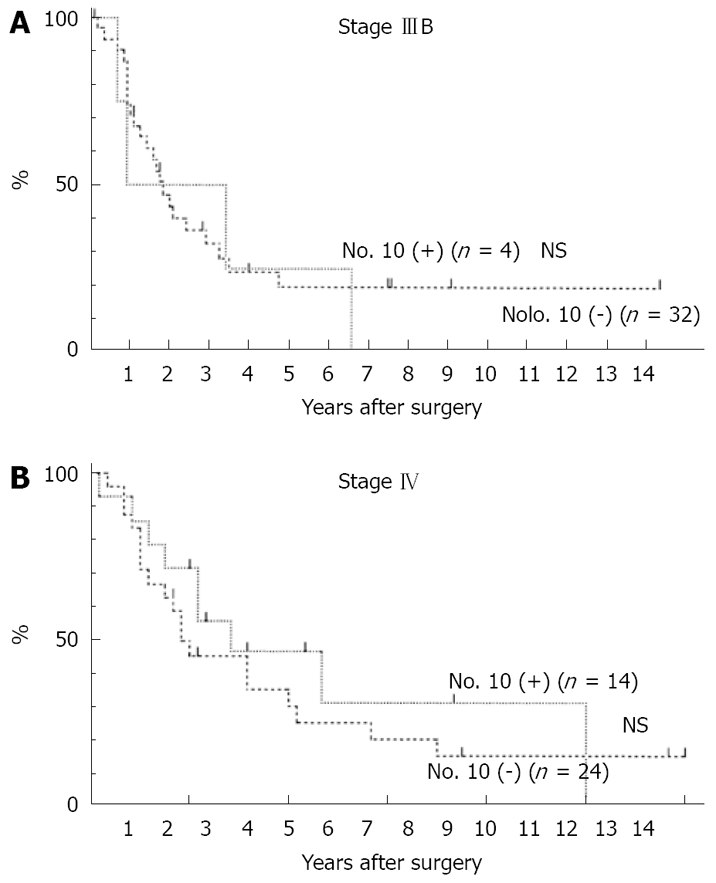
Methods: We studied 191 patients who had undergone total gastrectomy with splenectomy, excluding non-curative cases, resection of multiple gastric cancer, and those with remnant stomach cancer. Various clinicopathological factors were evaluated for any independent contributions to No. 10 LN metastasis, using χ(2) test. Significant factors were extracted for further analysis, carried out using a logistic regression method. Furthermore, lymph node metastasis was evaluated for any independent contribution to No. 10 LN metastasis, using the same methods. The cumulative survival rate was calculated using the Kaplan-Meier method. The significance of any difference between the survival curves was determined using the Cox-Mantel test, and any difference was considered significant at the 5% level.
Results: From the variables considered to be potentially associated with No. 10 LN metastasis, age, depth, invasion of lymph vessel, N factor, the number of lymph node metastasis, Stage, the number of sites, and location were found to differ significantly between those with metastasis (the Positive Group) and those without (the Negative Group). A logistic regression analysis showed that the localization and Stage were significant parameters for No. 10 LN metastasis. There was no case located on the lesser curvature in the Positive Group. The numbers of No. 2, No. 3, No. 4sa, No. 4sb, No. 4d, No. 7, and No. 11 LN metastasis were each found to differ significantly between the Positive Group and the Negative Group. A logistic regression analysis showed that No. 4sa, No. 4sb, and No. 11 LN metastasis were each a significant parameter for No. 10 LN metastasis. There was no significant difference in survival curves between the Positive Group and the Negative Group.
Conclusion: Splenectomy should be performed to dissect No. 10 LN for cases which have No. 4sa, No. 4sb or No. 11 LN metastasis. However, in cases where the tumor is located on the lesser curvature, splenectomy can be omitted.
Keywords: Gastric cancer; Lymph node metastasis; Lymphadenectomy, Splenectomy; Total gastrectomy.
Figures
References
-
- Japanese Gastric Cancer Association: Japanese classification of gastric carcinoma. 13th ed. Tokyo: Kanehara; 1999. pp. 6–16. - PubMed
-
- Chikara K, Hiroshi S, Masato N, Hirotoshi A, Goro M, Hidetaka O. Indications for pancreaticosplenectomy in advanced gastric cancer. Hepatogastroenterology. 2001;48:908–912. - PubMed
-
- Ikeguchi M, Kaibara N. Lymph node metastasis at the splenic hilum in proximal gastric cancer. Am Surg. 2004;70:645–648. - PubMed
-
- Fatouros M, Roukos DH, Lorenz M, Arampatzis I, Hottentrott C, Encke A, Kappas AM. Impact of spleen preservation in patients with gastric cancer. Anticancer Res. 2005;25:3023–3030. - PubMed
-
- Degiuli M, Sasako M, Ponzetto A, Allone T, Soldati T, Calgaro M, Balcet F, Bussone R, Olivieri F, Scaglione D, et al. Extended lymph node dissection for gastric cancer: results of a prospective, multi-centre analysis of morbidity and mortality in 118 consecutive cases. Eur J Surg Oncol. 1997;23:310–314. - PubMed
LinkOut - more resources
Full Text Sources
