

Acute esophageal variceal bleeding: Current strategies and new perspectives
- PMID: 21161008
- PMCID: PMC2998973
- DOI: 10.4254/wjh.v2.i7.261
Acute esophageal variceal bleeding: Current strategies and new perspectives
Abstract
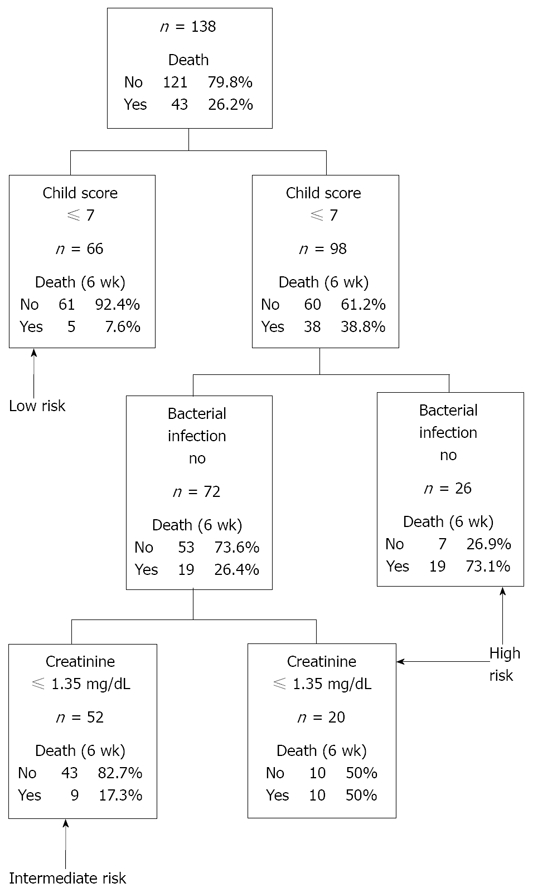
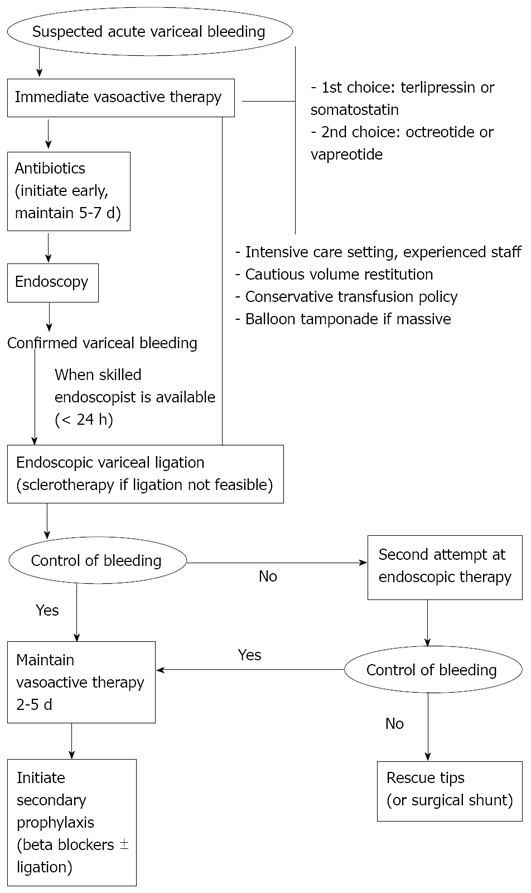
Management of acute variceal bleeding has greatly improved over recent years. Available data indicates that general management of the bleeding cirrhotic patient by an experienced multidisciplinary team plays a major role in the final outcome of this complication. It is currently recommended to combine pharmacological and endoscopic therapies for the initial treatment of the acute bleeding. Vasoactive drugs (preferable somatostatin or terlipressin) should be started as soon as a variceal bleeding is suspected (ideally during transfer to hospital) and maintained afterwards for 2-5 d. After stabilizing the patient with cautious fluid and blood support, an emergency diagnostic endoscopy should be done and, as soon as a skilled endoscopist is available, an endoscopic variceal treatment (ligation as first choice, sclerotherapy if endoscopic variceal ligation not feasible) should be performed. Antibiotic prophylaxis must be regarded as an integral part of the treatment of acute variceal bleeding and should be started at admission and maintained for at least 7 d. In case of failure to control the acute bleeding, rescue therapies should be immediately started. Shunt therapies (especially transjugular intrahepatic portosystemic shunt) are very effective at controlling treatment failures after an acute variceal bleeding. Therapeutic developments and increasing knowledge in the prognosis of this complication may allow optimization of the management strategy by adapting the different treatments to the expected risk of complications for each patient in the near future. Theoretically, this approach would allow the initiation of early aggressive treatments in high-risk patients and spare low-risk individuals unnecessary procedures. Current research efforts will hopefully clarify this hypothesis and help to further improve the outcomes of the severe complication of cirrhosis.
Keywords: Complications of cirrhosis; Portal hypertension; Variceal bleeding.
Figures
References
-
- Graham DY, Smith JL. The course of patients after variceal hemorrhage. Gastroenterology. 1981;80:800–809. - PubMed
-
- Gines P, Quintero E, Arroyo V, Teres J, Bruguera M, Rimola A. Compensated cirrhosis: natural history and prognostic factors. Hepatology. 1987;7:122–128. - PubMed
-
- El-Serag HB, Everhart JE. Improved survival after variceal hemorrhage over an 11-year period in the Department of Veterans Affairs. Am J Gastroenterol. 2000;95:3566–3573. - PubMed
-
- Augustin S, Muntaner L, Altamirano JT, González A, Saperas E, Dot J, Abu-Suboh M, Armengol JR, Malagelada JR, Esteban R, et al. Predicting early mortality after acute variceal hemorrhage based on classification and regression tree analysis. Clin Gastroenterol Hepatol. 2009;7:1347–1354. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
