

Superiority of moderate control of hyperglycemia to tight control in patients undergoing coronary artery bypass grafting
- PMID: 21163498
- PMCID: PMC3099050
- DOI: 10.1016/j.jtcvs.2010.10.005
Superiority of moderate control of hyperglycemia to tight control in patients undergoing coronary artery bypass grafting
Abstract
Objective: Although consensus in cardiac surgery supports tight control of perioperative hyperglycemia (glucose<120 mg/dL), recent studies in critical care suggest moderate glycemic control may be superior. We sought to determine whether tight control or moderate glycemic control is optimal after coronary artery bypass grafting.
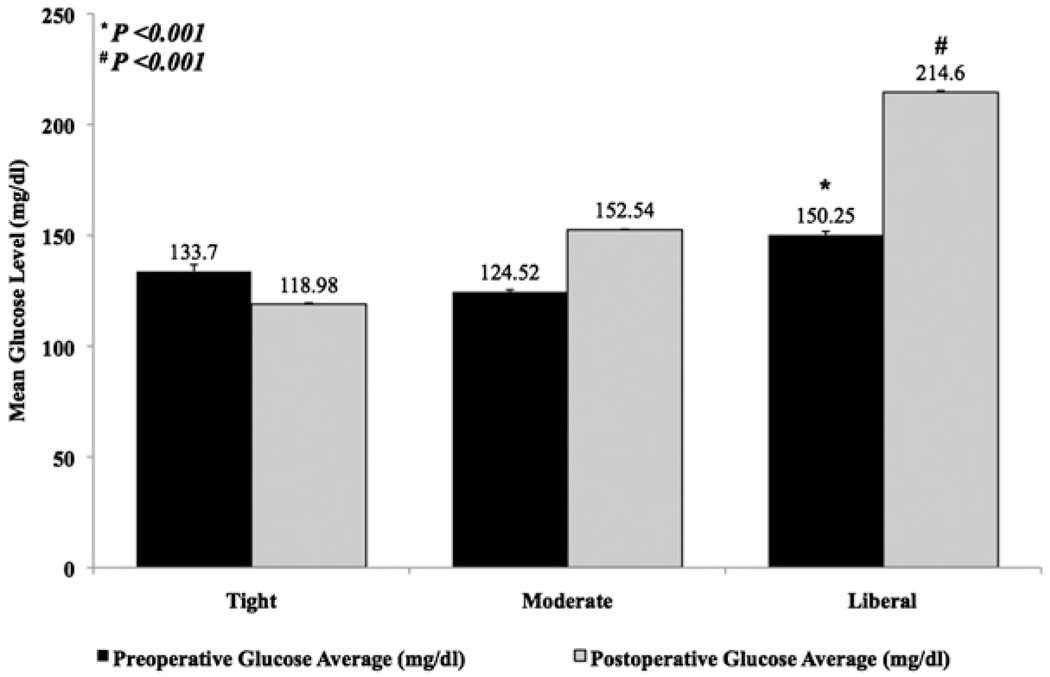
Methods: From 1995 to 2008, a total of 4658 patients with known diabetes or perioperative hyperglycemia (preoperative glycosylated hemoglobin≥8 or postoperative serum glucose>126 mg/dL) underwent isolated coronary artery bypass grafting at our institution. Patients were stratified into 3 postoperative glycemic groups: tight (≤126 mg/dL), moderate (127-179 mg/dL), and liberal (≥180 mg/dL). Preoperative risk factors, glycemic management, and postoperative outcomes were analyzed.
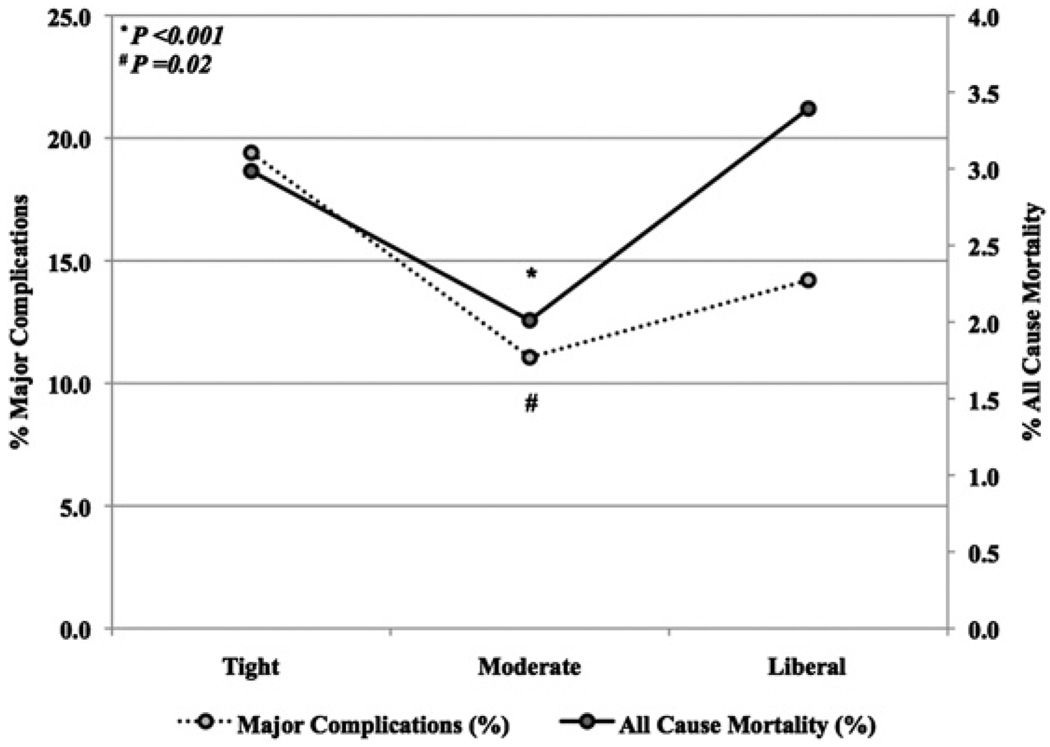
Results: Operative mortality was 2.5% (119/4658); major complication rate was 12.5% (581/4658). Relative to moderate group, more patients in tight group had preoperative renal failure (tight 16.4%, 22/134, moderate 8.3%, 232/2785, P=.001) and underwent emergent operations (tight 5.2%, 7/134, moderate 1.9%, 52/2785, P=.007); however, Society of Thoracic Surgeons predicted mortality risk was lower in tight group (P<.001). Moderate group had lowest mortality (tight 2.9%, 4/134, moderate 2.0%, 56/2785, liberal 3.4%, 59/1739, P=.02) and incidence of major complications (tight 19.4%, 26/134, moderate 11.1%, 308/2785, liberate 14.2%, 247/1739, P<.001). Risk-adjusted major complication incidence (adjusted odds ratio 0.7, 95% confidence interval 0.58-0.87) and mortality (adjusted odds ratio 0.6, 95% confidence interval 0.37-0.83) were lower with moderate glucose control than with tight or liberal management.
Conclusions: Moderate glycemic control was superior to tight glycemic control, with decreased mortality and major complications, and may be ideal for patients undergoing isolated coronary artery bypass grafting.
Copyright © 2011 The American Association for Thoracic Surgery. Published by Mosby, Inc. All rights reserved.
Figures
References
-
- Knapik P, Nadziakiewicz P, Urbanska E, Saucha W, Herdynska M, Zembala M. Cardiopulmonary bypass increases postoperative glycemia and insulin consumption after coronary surgery. Ann Thorac Surg. 2009;87:1859–1865. - PubMed
-
- Gandhi GY, Nuttall GA, Abel MD, Mullany CJ, Schaff HV, O’Brien PC, et al. Intensive intraoperative insulin therapy versus conventional glucose management during cardiac surgery: a randomized trial. Ann Intern Med. 2007;146:233–243. - PubMed
-
- Lecomte P, Foubert L, Nobels F, Coddens J, Nollet G, Casselman F, et al. Dynamic tight glycemic control during and after cardiac surgery is effective, feasible, and safe. Anesth Analg. 2008;107:51–58. - PubMed
-
- Zerr KJ, Furnary AP, Grunkemeier GL, Bookin S, Kanhere V, Starr A. Glucose control lowers the risk of wound infection in diabetics after open heart operations. Ann Thorac Surg. 1997;63:356–361. - PubMed
