

Optimism bias leads to inconclusive results-an empirical study
- PMID: 21163620
- PMCID: PMC3079810
- DOI: 10.1016/j.jclinepi.2010.09.007
Optimism bias leads to inconclusive results-an empirical study
Abstract
Objective: Optimism bias refers to unwarranted belief in the efficacy of new therapies. We assessed the impact of optimism bias on a proportion of trials that did not answer their research question successfully and explored whether poor accrual or optimism bias is responsible for inconclusive results.
Study design: Systematic review.
Setting: Retrospective analysis of a consecutive-series phase III randomized controlled trials (RCTs) performed under the aegis of National Cancer Institute Cooperative groups.
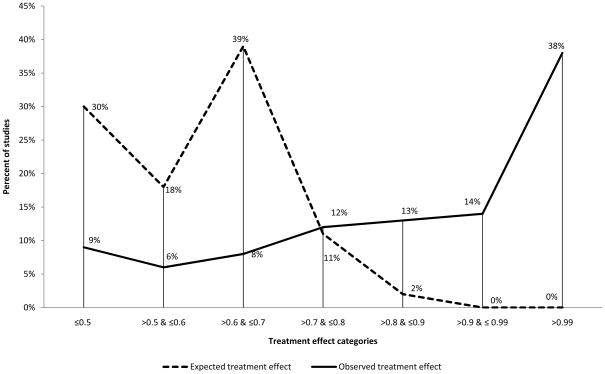
Results: Three hundred fifty-nine trials (374 comparisons) enrolling 150,232 patients were analyzed. Seventy percent (262 of 374) of the trials generated conclusive results according to the statistical criteria. Investigators made definitive statements related to the treatment preference in 73% (273 of 374) of studies. Investigators' judgments and statistical inferences were concordant in 75% (279 of 374) of trials. Investigators consistently overestimated their expected treatment effects but to a significantly larger extent for inconclusive trials. The median ratio of expected and observed hazard ratio or odds ratio was 1.34 (range: 0.19-15.40) in conclusive trials compared with 1.86 (range: 1.09-12.00) in inconclusive studies (P<0.0001). Only 17% of the trials had treatment effects that matched original researchers' expectations.
Conclusion: Formal statistical inference is sufficient to answer the research question in 75% of RCTs. The answers to the other 25% depend mostly on subjective judgments, which at times are in conflict with statistical inference. Optimism bias significantly contributes to inconclusive results.
Copyright © 2011 Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures







References
-
-
http://www.wma.net/e/policy/b3.htm. [cited; Available from:
-
-
- World Medical Association. World Medical Association Declaration of Helskinki. Ethical Principles for Medical Research Involving Human Subjects. 2007. [cited 2008 20th October]; Available from: http://www.wma.net/e/policy/b3.htm.
-
- Edwards SJL, Lilford RJ, Braunholtz DA, Jackson JC, Hewison J, Thornton J. Ethical issues in the design and conduct of randomized controlled trials. Health Technol Assessment. 1998;2(15):1–130. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
