

Multiresistant bacteria and current therapy - the economical side of the story
- PMID: 21163732
- PMCID: PMC3352106
- DOI: 10.1186/2047-783x-15-12-571
Multiresistant bacteria and current therapy - the economical side of the story
Abstract
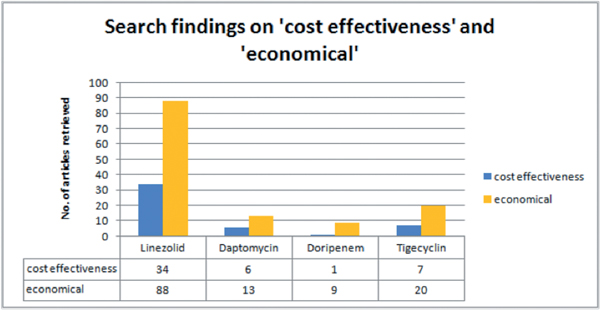
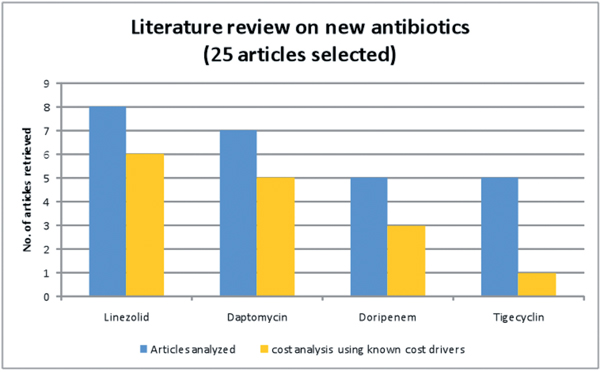
Severe infections with multiresistant bacteria (MRB) are a medical challenge and a financial burden for hospitals. The adequate antibiotic therapy is a key issue in multiresistant bacteria management. Several major cost drivers have been identified. Remarkably drug acquisition costs are not necessarily included. Most significant are the length of stay in hospital, the hours of mechanical ventilation and the time treated on an intensive care unit. - In a systematic review of the literature the following aspects were investigated: - Do generic treatment strategies contribute in cost savings? - Are there specific results for recent antibiotics? - Early adequate and effective antimicrobial treatment, switch from i.v. to oral therapy, adjusted duration of therapy and adherence to guidelines have been found to be successful strategies. - Looking at specific antibiotics, the best evidence for cost-effectiveness is found for Linezolid in treatment of cSSTI as well as in HAP. Daptomycin shows good economic results in bloodstream infections, so possibly being a cost-effective alternative to vancomycin. Looking at tigecycline the published data show neither higher costs nor savings compared to imipeneme. Doripenem as one of the newest therapy options has proven to be highly cost-saving in HAP when compared with imipenem. However, most analyses are based on pharmacoeconomic modelling rather than on directly analysing trial data or real life clinical populations. -
Conclusion: Using modern antibiotics in whole is not more expensive than using established therapies. Modern antibiotics are cost-effective and sometimes even cost-saving. This is especially true if an effective therapy is initiated as early as possible.
Figures
References
-
- Köck R. et al. Methicillin-resistant Staphylococcus aureus (MRSA): burden of disease and control challenges in Europe. Euro Surveill. 2010;15(41):19688. - PubMed
-
- Schweickert B, The MRSA-Import in ICUs is an important predictor for the occurrence of nosocomial MRSA-cases. Clin Microbiol Infect. 2010. in press doi: 10.1111/j.1469-0691.2010.03409.x. - PubMed
-
- Resch A, Wilke M, Fink C. The cost of resistance: incremental cost of methicillin-resistant Staphylococcus aureus (MRSA) in German hospitals. Eur J Health Econ. 2009;10(1):287–97. - PubMed
-
- Wernitz MH, Lenz C, Veit SK. Die Bedeutung von Infektionen durch multiresistente Staphylococcus aureus für das deutsche Gesundheitswesen - The (n)ever ending story? J Pharmakol Ther. 2009;18:75–82.
-
- Ott E, Costs of nosocomial pneumonia caused by meticillin-resistant Staphylococcus aureus. J Hosp Infect. 2010. in press . - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
