

Effectiveness of a web-based intervention for problem drinkers and reasons for dropout: randomized controlled trial
- PMID: 21163776
- PMCID: PMC3056532
- DOI: 10.2196/jmir.1642
Effectiveness of a web-based intervention for problem drinkers and reasons for dropout: randomized controlled trial
Abstract
Background: Online self-help interventions for problem drinkers show promising results, but the effectiveness of online therapy with active involvement of a therapist via the Internet only has not been examined.
Objective: The objective of our study was to evaluate an e-therapy program with active therapeutic involvement for problem drinkers, with the hypotheses that e-therapy would (1) reduce weekly alcohol consumption, and (2) improve health status. Reasons for dropout were also systematically investigated.
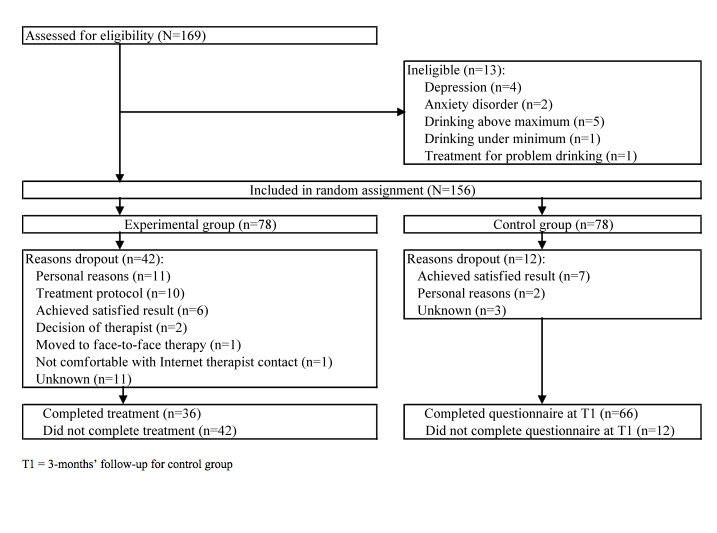
Method: In an open randomized controlled trial, Dutch-speaking problem drinkers in the general population were randomly assigned (in blocks of 8, according to a computer-generated random list) to the 3-month e-therapy program (n = 78) or the waiting list control group (n = 78). The e-therapy program consisted of a structured 2-part online treatment program in which the participant and the therapist communicated asynchronously, via the Internet only. Participants in the waiting list control group received "no-reply" email messages once every 2 weeks. The primary outcome measures were (1) the difference in the score on weekly alcohol consumption, and (2) the proportion of participants drinking under the problem drinking limit. Intention-to-treat analyses were performed using multiple imputations to deal with loss to follow-up. A dropout questionnaire was sent to anyone who did not complete the 3-month assessment. Reasons for dropout were independently assessed by the first and third author.
Results: Of the 156 individuals who were randomly assigned, 102 (65%) completed assessment at 3 months. In the intention-to-treat analyses, the e-therapy group (n = 78) showed a significantly greater decrease in alcohol consumption than those in the control group (n = 78) at 3 months. The e-therapy group decreased their mean weekly alcohol consumption by 28.8 units compared with 3.1 units in the control group, a difference in means of 25.6 units on a weekly basis (95% confidence interval 15.69-35.80, P < .001). The between-group effect size (pooled SD) was large (d = 1.21). The results also showed that 68% (53/78) of the e-therapy group was drinking less than 15 (females) or 22 (males) units a week, compared with 15% (12/78) in the control group (OR 12.0, number needed to treat 1.9, P < .001). Dropout analysis showed that the main reasons for dropouts (n = 54) were personal reasons unrelated to the e-therapy program, discomfort with the treatment protocol, and satisfaction with the positive results achieved.
Conclusions: E-therapy for problem drinking is an effective intervention that can be delivered to a large population who otherwise do not seek help for their drinking problem. Insight into reasons for dropout can help improve e-therapy programs to decrease the number of dropouts. Additional research is needed to directly compare the effectiveness of the e-therapy program with a face-to-face treatment program.
Conflict of interest statement
None declared
Figures

References
-
- Smit F, Cuijpers P, Oostenbrink J, Batelaan N, de Graaf R, Beekman A. Costs of nine common mental disorders: implications for curative and preventive psychiatry. J Ment Health Policy Econ. 2006 Dec;9(4):193–200. - PubMed
-
- Cunningham JA, Breslin FC. Only one in three people with alcohol abuse or dependence ever seek treatment. Addict Behav. 2004 Jan;29(1):221–3.S0306460303000777 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
