

Feedback GAP: study protocol for a cluster-randomized trial of goal setting and action plans to increase the effectiveness of audit and feedback interventions in primary care
- PMID: 21167034
- PMCID: PMC3161381
- DOI: 10.1186/1748-5908-5-98
Feedback GAP: study protocol for a cluster-randomized trial of goal setting and action plans to increase the effectiveness of audit and feedback interventions in primary care
Abstract
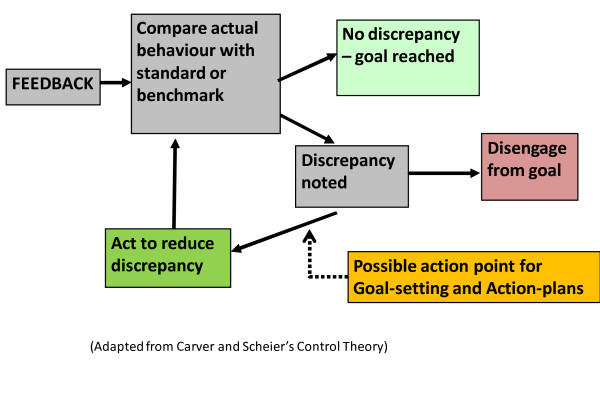
Background: Audit and feedback to physicians is commonly used alone or as part of multifaceted interventions. While it can play an important role in quality improvement, the optimal design of audit and feedback is unknown. This study explores how feedback can be improved to increase acceptability and usability in primary care. The trial seeks to determine whether a theory-informed worksheet appended to feedback reports can help family physicians improve quality of care for their patients with diabetes and/or ischemic heart disease.
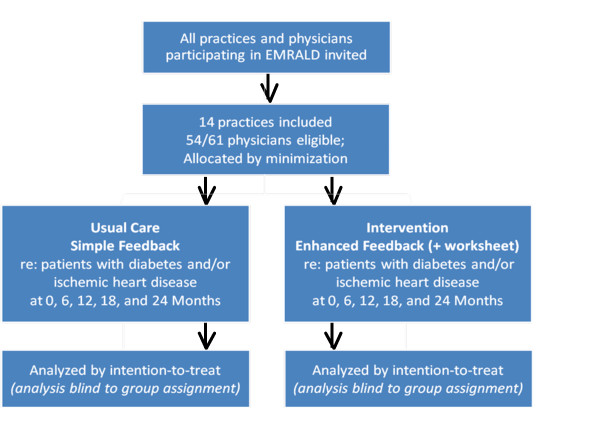
Methods: Two-arm cluster trial was conducted with participating primary care practices allocated using minimization to simple feedback or enhanced feedback group. The simple feedback group receives performance feedback reports every six months for two years regarding the proportion of their patients with diabetes and/or ischemic heart disease who are meeting quality targets. The enhanced feedback group receives these same reports as well as a theory-informed worksheet designed to facilitate goal setting and action plan development in response to the feedback reports. Participants are family physicians from across Ontario who use electronic medical records; data for rostered patients are used to produce the feedback reports and for analysis.
Outcomes: The primary disease outcomes are the blood pressure (BP), and low-density lipoprotein cholesterol (LDL) levels. The primary process measure is a composite score indicating the number of recommended activities (e.g., tests and prescriptions) conducted by the family physicians for their patients with diabetes and/or ischemic heart disease within the appropriate timeframe. Secondary outcomes are the proportion of patients whose results meet targets for glucose, LDL, and BP as well as the percent of patients receiving relevant prescriptions. A qualitative process evaluation using semi-structured interviews will explore perceived barriers to behaviour change in response to feedback reports and preferences with regard to feedback design.
Analysis: Intention-to-treat approach will be used to analyze the trial. Analysis will be performed on patient-level variables using generalized estimating equation models to adjust for covariates and account for the clustered nature of the data. The trial is powered to show small, but clinically important differences of 7 mmHG in systolic BP and 0.32 mmol/L in LDL.
Trial registration: ClinicalTrials.gov NCT00996645.
Figures
References
-
- Narayan KM, Benjamin E, Gregg EW, Norris SL, Engelgau MM. Diabetes translation research: where are we and where do we want to be? Ann Intern Med. 2004;140(11):958–963. - PubMed
-
- Davis D, Davis N. In: Knowledge Translation in Health Care - Moving from Evidence to Practice. Straus S, Tetroe J, Graham ID, editor. UK: Wiley-Blackwell; 2009. Educational Interventions; p. 116.
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
