

Multiple pudendal sensory pathways reflexly modulate bladder and urethral activity in patients with spinal cord injury
- PMID: 21168860
- PMCID: PMC3056321
- DOI: 10.1016/j.juro.2010.09.079
Multiple pudendal sensory pathways reflexly modulate bladder and urethral activity in patients with spinal cord injury
Abstract
Purpose: Electrical stimulation of pudendal afferents can evoke reflex bladder contractions with relaxation of the external urethral sphincter in cats. This voiding reflex is mediated by pudendal sensory fibers innervating the penile and prostatic urethra that engage spinal and spinobulbospinal micturition pathways, respectively. However, clinical translation of this potential therapy in individuals with spinal cord injury is limited by the lack of evidence showing analogous reflex mechanisms in humans. We investigated excitatory pudendal-to-bladder reflexes in 7 individuals with chronic spinal cord injury.
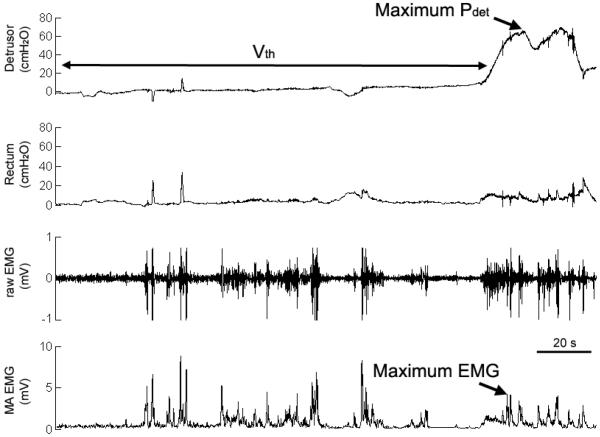
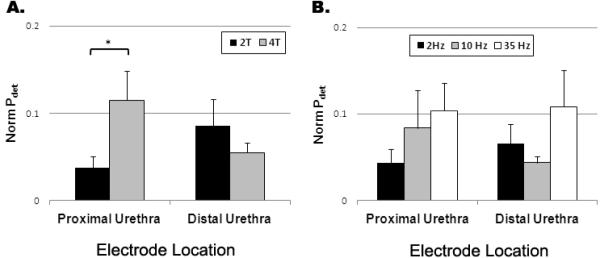
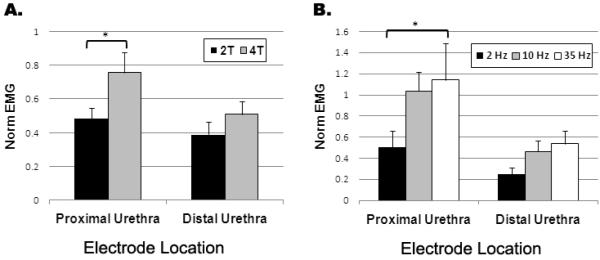
Materials and methods: We recorded isovolumetric bladder pressure and perineal electromyogram in response to intraurethral electrical stimulation at varying amplitudes and frequencies.
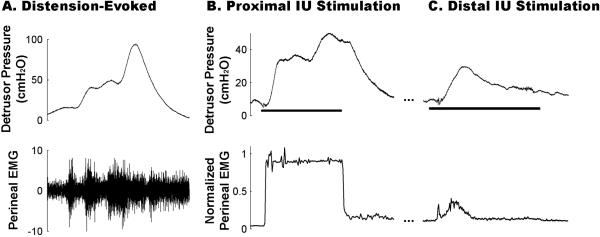
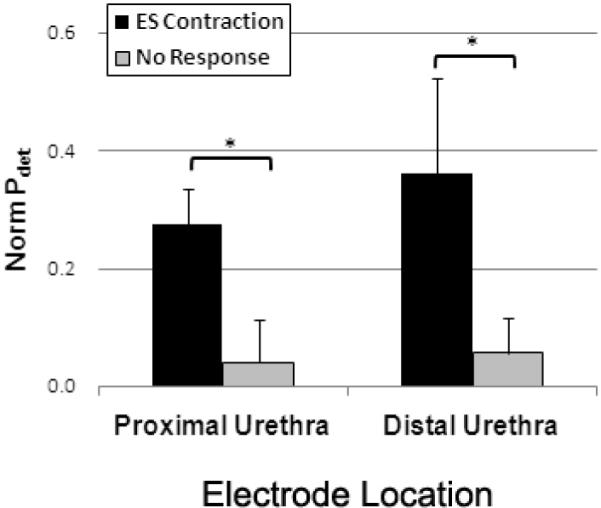
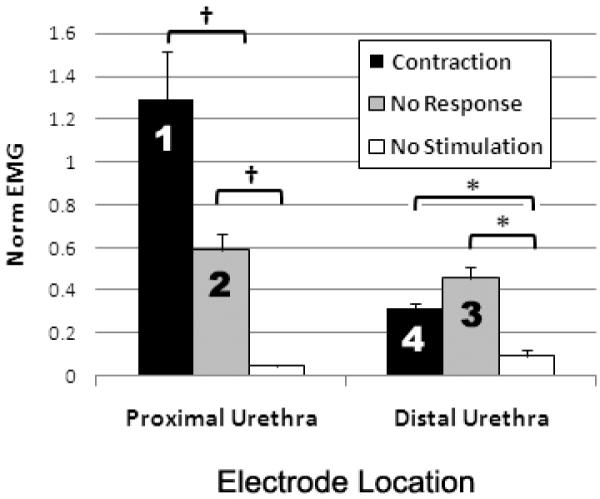
Results: Selective electrical stimulation of the proximal (29.7 ± 11.6 cm H(2)O) and distal urethral (23.3 ± 9.28 cm H(2)O) segments evoked sustained reflex bladder contractions in different subsets (3 each) of participants. In contrast, the corresponding reflex perineal electromyogram revealed a differential activation pattern between proximal and distal intraurethral stimulation (normalized electromyogram of 1.3 ± 0.2 and 0.3 ± 0.1, respectively, p <0.05).
Conclusions: To our knowledge we report the first clinical evidence of 2 independent excitatory pudendal-to-bladder reflex pathways, which in turn differentially modulate efferent pudendal output. Each reflex mechanism involves complex interaction of multiple sensory inputs and may provide a neural substrate to restore micturition after spinal cord injury.
Copyright © 2011 American Urological Association Education and Research, Inc. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Benevento BT, Sipski ML. Neurogenic bladder, neurogenic bowel, and sexual dysfunction in people with spinal cord injury. Phys Ther. 2002;82:601. - PubMed
-
- de Groat WC, Araki I, Vizzard MA, et al. Developmental and injury induced plasticity in the micturition reflex pathway. Behav Brain Res. 1998;92:127. - PubMed
-
- Shingleton WB, Bodner DR. The development of urologic complications in relationship to bladder pressure in spinal cord injured patients. J Am Paraplegia Soc. 1993;16:14. - PubMed
-
- Tai C, Wang J, Wang X, et al. Bladder inhibition or voiding induced by pudendal nerve stimulation in chronic spinal cord injured cats. Neurourol Urodyn. 2007;26:570. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
