

Pituitary surgery for small prolactinomas as an alternative to treatment with dopamine agonists
- PMID: 21170594
- PMCID: PMC3146980
- DOI: 10.1007/s11102-010-0283-y
Pituitary surgery for small prolactinomas as an alternative to treatment with dopamine agonists
Abstract
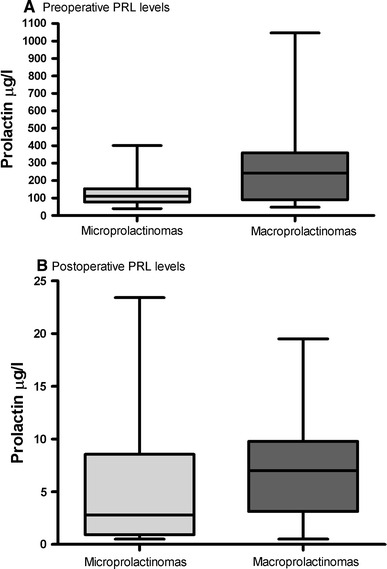
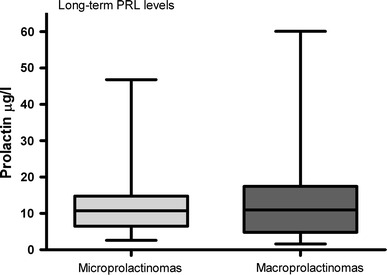
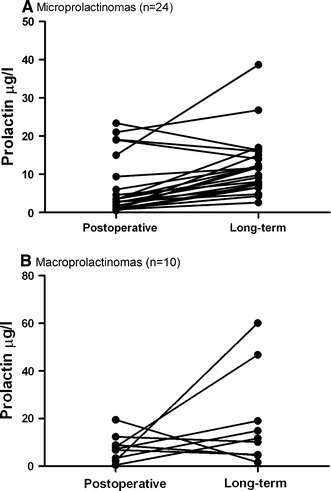
Despite the fact that consensus guidelines recommend long-term dopamine agonist (DA) therapy as a first-line approach to the treatment of small prolactinoma, some patients continue to prefer a primary surgical approach. Concerns over potential adverse effects of long-term medical therapy and/or the desire to become pregnant and avoid long-term medication are often mentioned as reasons to pursue surgical removal. In this retrospective study, 34 consecutive patients (30 female, 4 male) preferably underwent primary pituitary surgery without prior DA treatment for small prolactinomas (microprolactinoma 1-10 mm, macroprolactinoma 11-20 mm) at the Department of Neurosurgery, University of Bern, Switzerland. At the time of diagnosis, 31 of 34 patients (91%) presented with symptoms. Patients with microprolactinomas had significantly lower preoperative prolactin (PRL) levels compared to patients with macroprolactinomas (median 143 μg/l vs. 340 μg/l). Ninety percent of symptomatic patients experienced significant improvement of their signs and symptoms upon surgery. The postoperative PRL levels (median 3.45 μg/l) returned to normal in 94% of patients with small prolactinomas. There was no mortality and no major morbidities. One patient suffered from hypogonadotropic hypogonadism after surgery despite postoperative normal PRL levels. Long-term remission was achieved in 22 of 24 patients (91%) with microprolactinomas, and in 8 of 10 patients (80%) with macroprolactinomas after a median follow-up period of 33.5 months. Patients with small prolactinomas can safely consider pituitary surgery in a specialized centre with good chance of long-term remission as an alternative to long-term DA therapy.
Conflict of interest statement
The authors have nothing to disclose and no conflict of interest.
Figures
Comment in
-
Re.: Pituitary surgery for small prolactinomas as an alternative to treatment with dopamine agonists.J Urol. 2011 May;185(5):1836-7. doi: 10.1016/S0022-5347(11)60218-8. J Urol. 2011. PMID: 22088729 No abstract available.
References
-
- Molitch ME (1999) Medical treatment of prolactinomas. Endocrinol Metab Clin North Am 28(1):143–169 - PubMed
-
- Casanueva FF, Molitch ME, Schlechte JA, Abs R, Bonert V, Bronstein MD et al (2006) Guidelines of the pituitary society for the diagnosis and management of prolactinomas. Clin Endocrinol (Oxf) 65(2):265–273 - PubMed
-
- Gillam MP, Molitch ME, Lombardi G, Colao A (2006) Advances in the treatment of prolactinomas. Endocr Rev 27(5):485–534 - PubMed
-
- Dekkers OM, Lagro J, Burman P, Jorgensen JO, Romijn JA, Pereira AM (2009) Recurrence of hyperprolactinemia after withdrawal of dopamine agonists: systematic review and meta-analysis. J Clin Endocrinol Metab 95(1):43–51 - PubMed
-
- Verhelst J, Abs R, Maiter D, van den Bruel A, Vandeweghe M, Velkeniers B et al (1999) Cabergoline in the treatment of hyperprolactinemia: a study in 455 patients. J Clin Endocrinol Metab 84(7):2518–2522 - PubMed
