

Contribution of sedative-hypnotic agents to delirium via modulation of the sleep pathway
- PMID: 21170622
- PMCID: PMC3033507
- DOI: 10.1007/s12630-010-9421-2
Contribution of sedative-hypnotic agents to delirium via modulation of the sleep pathway
Abstract
Purpose: To review the mechanisms of sedative-hypnotic action with respect to the risk of delirium imparted by drugs that act on γ-amino-butyric-acid type A receptors or α(2) adrenoceptors.
Source: MEDLINE was searched for relevant articles.
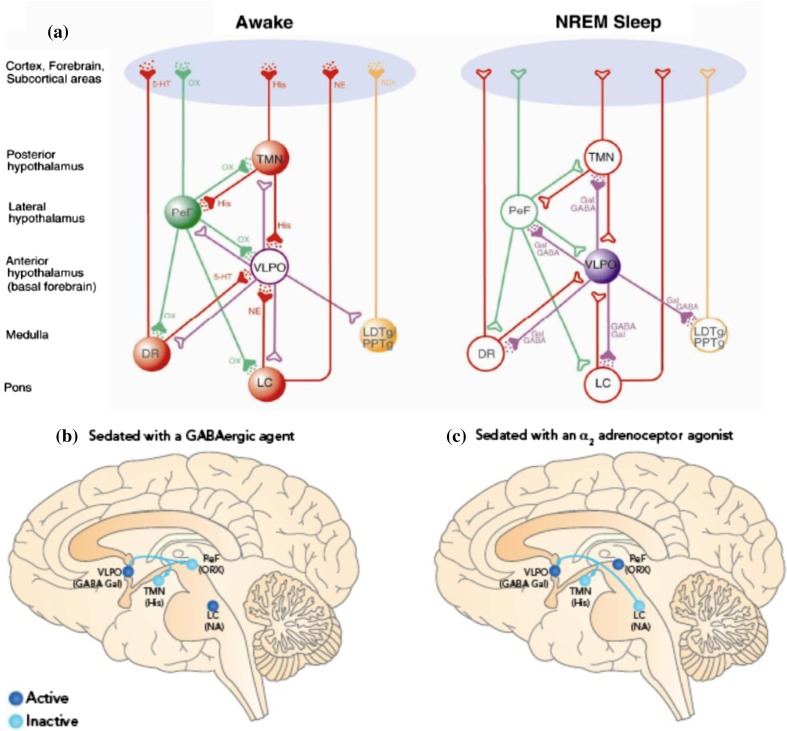
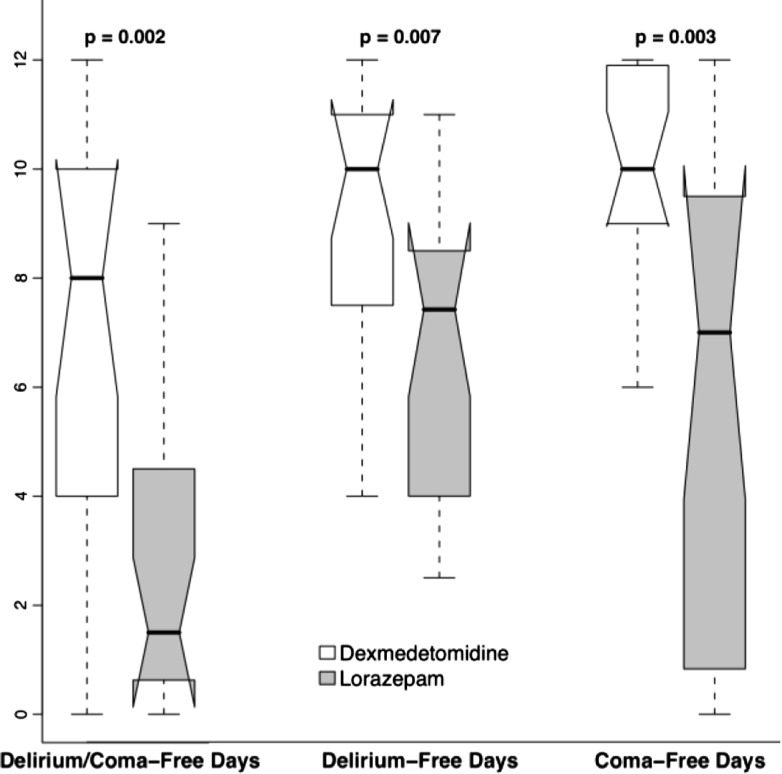
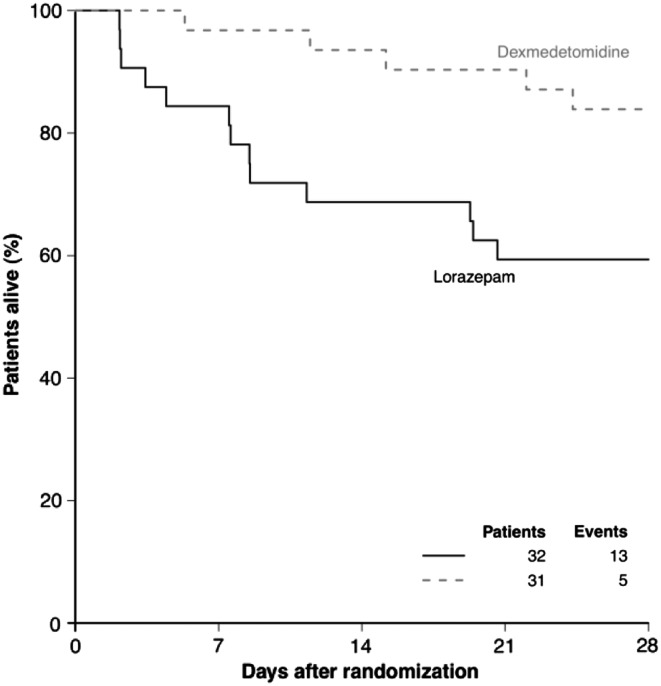
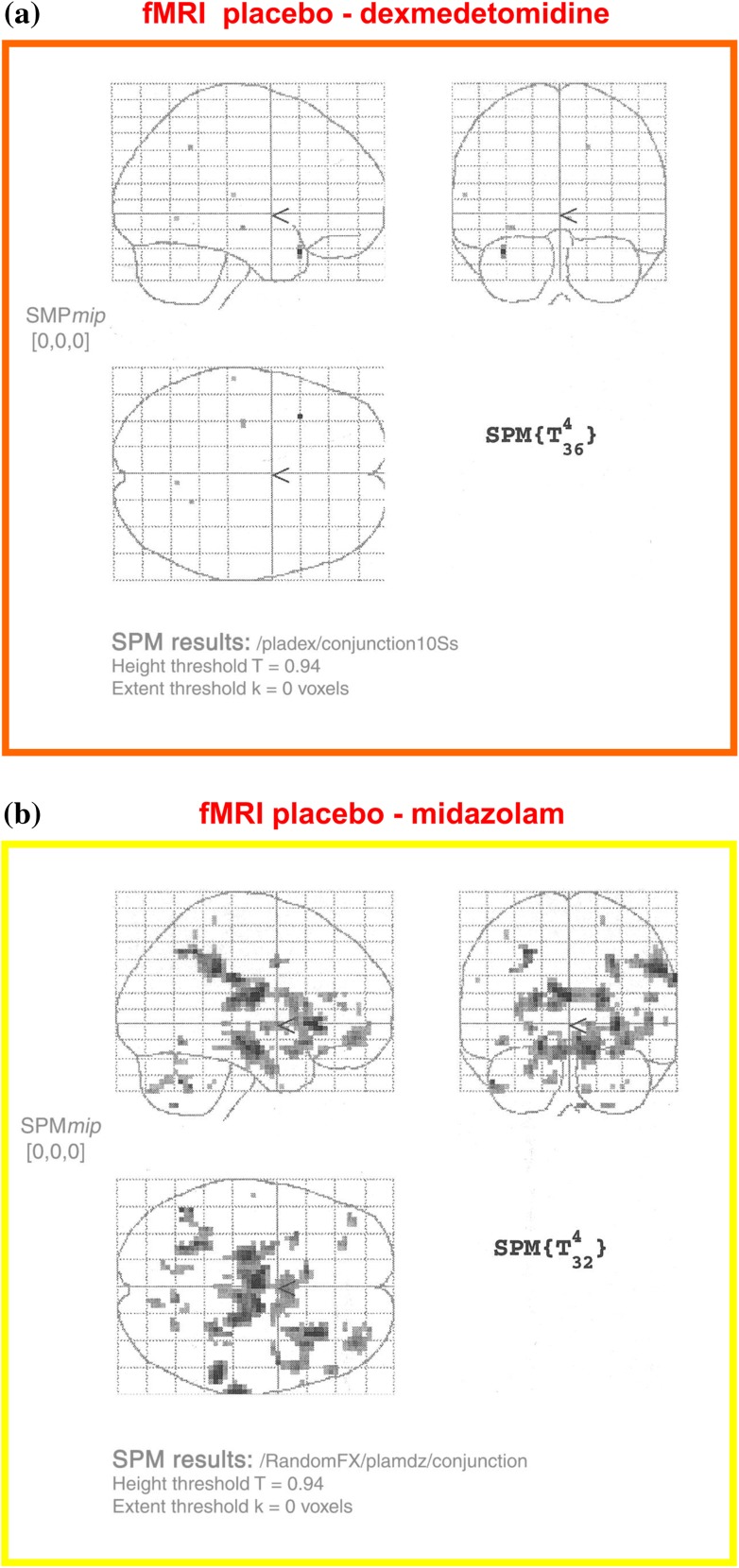
Principal findings: Development of the acute confusional state of delirium is associated with longer intensive care unit (ICU) and hospital lengths of stay, significantly higher risk of functional decline, and increased mortality. Disruption of sleep is a modifiable risk factor that may contribute to delirium and cognitive dysfunction in ICU patients. Among the functions of sleep are repair of defective processes and restoration of the brain to a state in which it is ready to acquire new knowledge. It is logical that disruption of these processes may produce acute confusion. Delirium develops through a complex interaction between the patient's baseline vulnerability (patient's predisposing risk factors before hospitalization) and precipitating factors or insults (modifiable events that occur during hospitalization). The latter factors include both sleep disruption and sedation. We present a hypothesis that these two factors are causally linked through effects on memory. Our hypothesis explains why patients randomized to receive an α(2) adrenoceptor agonist are less likely to develop delirium (and the attendant cognitive dysfunction) than those randomized to receive benzodiazepines.
Conclusion: Herein we present our hypothesis that alternate mechanisms of hypnotic action may differentiate the deleriogenic properties of the two classes of sedatives. Future studies should focus on whether a causal relationship can be established between sedative administration, sleep disruption, and delirium.
Objectif: Passer en revue les mécanismes d’action sédatifs-hypnotiques par rapport au risque de delirium imparti par les médicaments qui agissent sur les récepteurs de l’acide γ-amino-butyrique de type A (GABAA) et les adrénocepteurs α2.
Source: Une recherche a été effectuée dans la base de données MEDLINE pour en extraire les articles pertinents.
Constatations principales: L’apparition d’un état de confusion aigu de delirium est associée à des durées prolongées de séjour à l’unité des soins intensifs (USI) et à l’hôpital, à un risque significativement plus élevé de déclin fonctionnel et à une mortalité accrue. La perturbation du sommeil est un facteur de risque modifiable qui pourrait contribuer au delirium et à la dysfonction cognitive chez les patients de l’USI. La réparation des processus déficients et le rétablissement du cerveau à un état préparé à acquérir de nouvelles connaissances sont certaines des fonctions du sommeil. Il est logique que la perturbation de ces processus puisse provoquer une confusion aiguë. Le delirium survient suite à une interaction complexe entre la vulnérabilité fondamentale du patient (les facteurs de risque avant l’hospitalisation prédisposant le patient au delirium) et des facteurs ou lésions précipitants (événements modifiables survenant pendant l’hospitalisation). Ces seconds facteurs comprennent les perturbations du sommeil et la sédation. Nous présentons l’hypothèse que ces deux facteurs ont un lien de causalité par le biais d’effets sur la mémoire. Notre hypothèse explique pourquoi il est moins probable que des patients randomisés à recevoir un agoniste de l’adrénocepteur α2 manifestent un delirium (et la dysfonction cognitive concomitante) que des patients randomisés à recevoir des benzodiazépines.
Conclusion: Nous présentons ici notre hypothèse selon laquelle des mécanismes d’action hypnotique différents pourraient permettre de distinguer les propriétés délirogènes des deux classes de sédatifs. Les études devraient à l’avenir essayer de déterminer s’il existe une relation de causalité entre l’administration de sédatifs, les perturbations du sommeil et le delirium.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
