

Folic acid and prevention of colorectal adenomas: a combined analysis of randomized clinical trials
- PMID: 21170989
- PMCID: PMC3753215
- DOI: 10.1002/ijc.25872
Folic acid and prevention of colorectal adenomas: a combined analysis of randomized clinical trials
Abstract
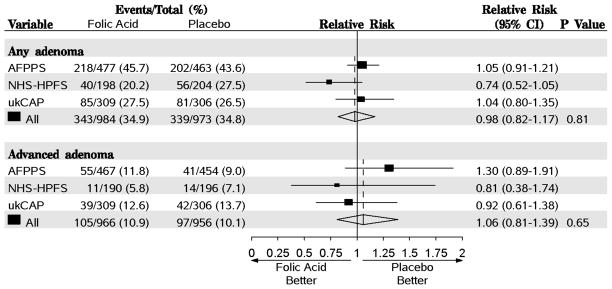
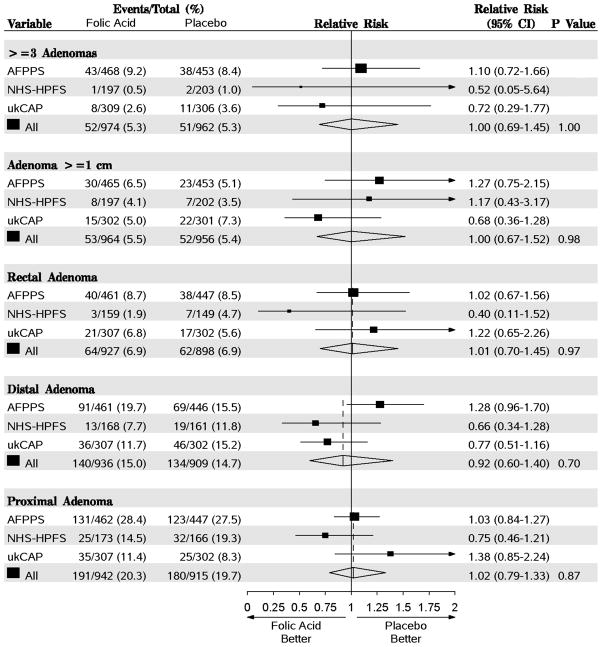
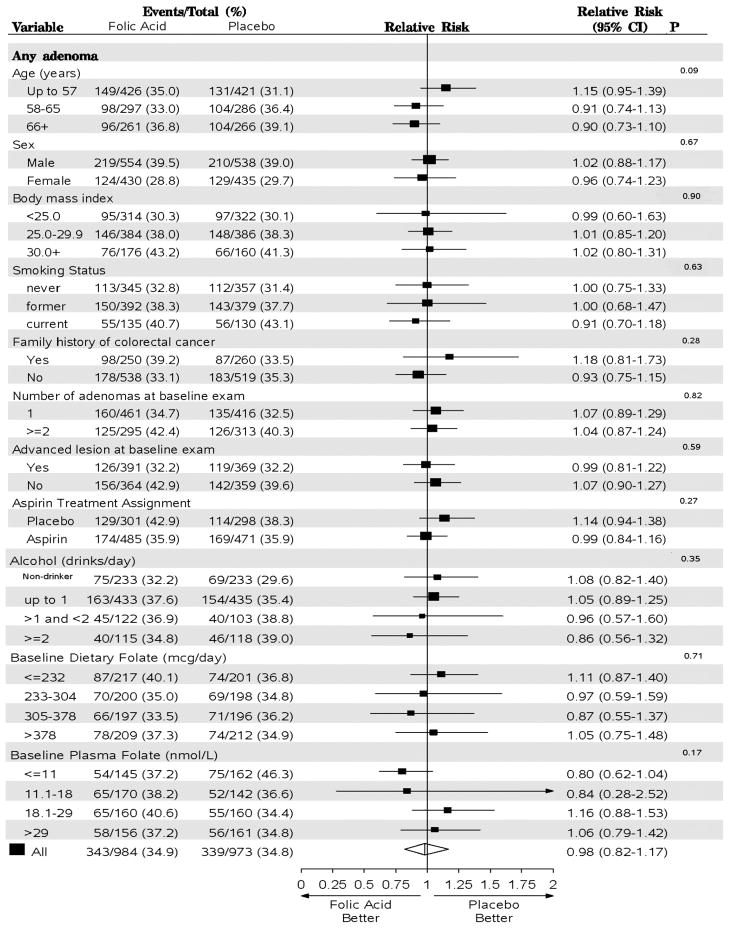
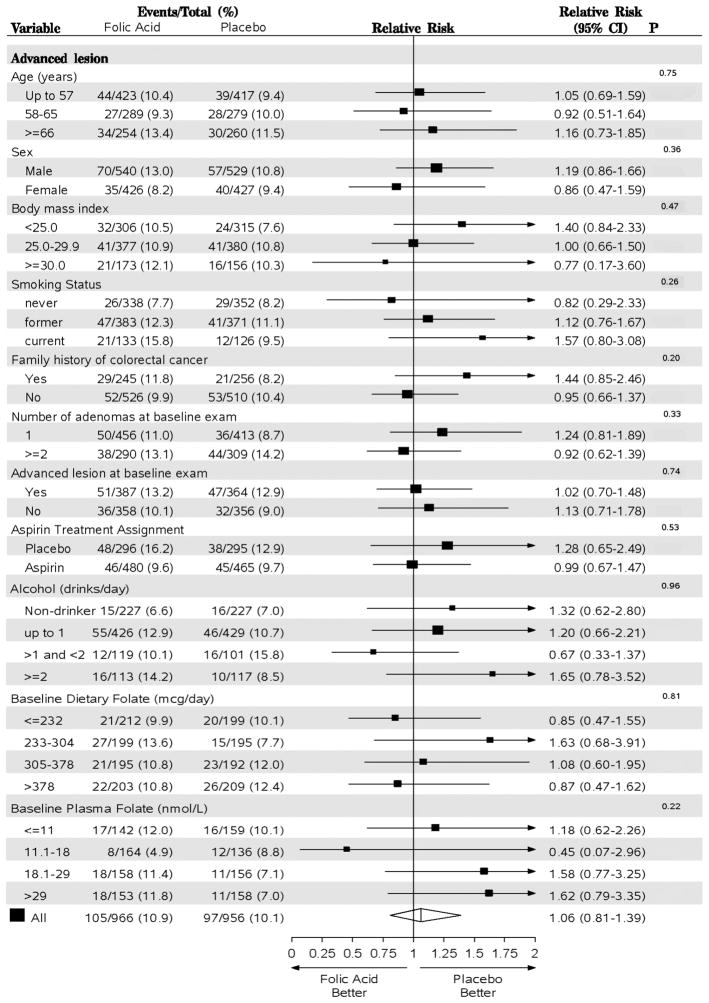
Observational data suggest that lower folate status is associated with an increased risk of colorectal neoplasia, implying that folate may be useful as a chemopreventive agent. We conducted a combined analysis of three large randomized trials of folic acid supplementation for the prevention of metachronous adenomas in patients with an adenoma history. Participants included 2,632 men and women who had a history of adenomas randomized to either 0.5 or 1.0 mg/day of folic acid or placebo and who had a follow-up endoscopy 6 to 42 months after randomization [mean = 30.6 (standard deviation = 8.1) months]. We used random-effects meta-analysis to estimate risk ratios (RRs) and 95% confidence intervals (CIs). The RR comparing folic acid versus placebo was 0.98 (95% CI = 0.82-1.17) for all adenomas and 1.06 (95% CI = 0.81-1.39) for advanced lesions. Folic acid was associated with a nonsignificant decreased risk of any adenoma among subjects in the lowest quartile of baseline plasma folate (≤ 11 nmol/L) and no effect among individuals in the highest quartile (> 29 nmol/L, p for trend = 0.17). There was a nonsignificant trend of decreasing risk of any adenoma associated with folic acid supplements with increasing alcohol intake. During the early follow-up reported here, more deaths occurred in the placebo group than in the folic acid group (1.7% vs. 0.5%, p = 0.002). In conclusion, after up to 3.5 years of folic acid use, there is no clear decrease or increase in the occurrence of new adenomas in patients with a history of adenoma.
Copyright © 2010 UICC.
Figures
References
-
- Giovannucci E. Epidemiologic studies of folate and colorectal neoplasia: a review. J Nutr. 2002;132:2350S–5S. - PubMed
-
- Sanjoaquin MA, Allen N, Couto E, Roddam AW, Key TJ. Folate intake and colorectal cancer risk: a meta-analytical approach. Int J Cancer. 2005;113:825–8. - PubMed
-
- Mason JB, Dickstein A, Jacques PF, Haggarty P, Selhub J, Dallal G, Rosenberg IH. A temporal association between folic acid fortification and an increase in colorectal cancer rates may be illuminating important biological principles: a hypothesis. Cancer Epidemiol Biomarkers Prev. 2007;16:1325–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
