

Improved prognosis for older adolescents with acute lymphoblastic leukemia
- PMID: 21172890
- PMCID: PMC3058285
- DOI: 10.1200/JCO.2010.32.0325
Improved prognosis for older adolescents with acute lymphoblastic leukemia
Abstract
Purpose: The prognosis for older adolescents and young adults with acute lymphoblastic leukemia (ALL) has been historically much worse than that for younger patients. We reviewed the outcome of older adolescents (age 15 to 18 years) treated in four consecutive Total Therapy studies to determine if recent improved treatment extended to this high-risk group.
Patients and methods: Between 1991 and 2007, 963 pediatric patients, including 89 older adolescents, were enrolled on Total Therapy studies XIIIA, XIIIB, XIV, and XV. In the first three studies, treatment selection was based on presenting clinical features and leukemic cell genetics. In study XV, the level of residual disease was used to guide treatment, which featured intensive methotrexate, glucocorticoid, vincristine, and asparaginase, as well as early triple intrathecal therapy for higher-risk ALL.
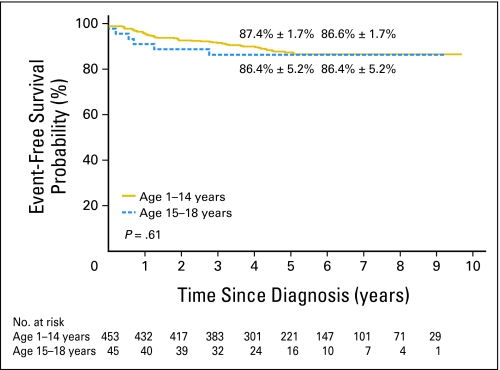
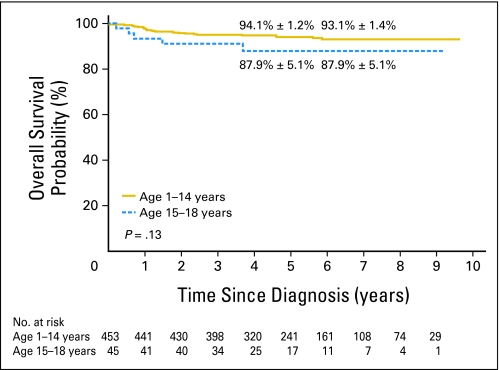
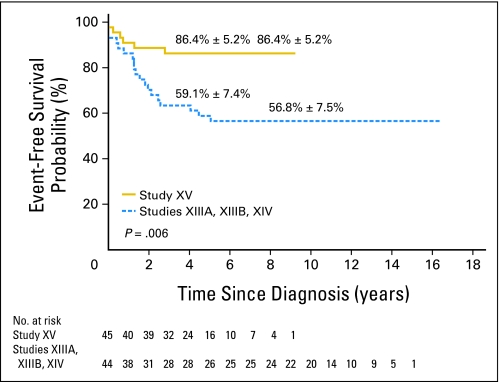
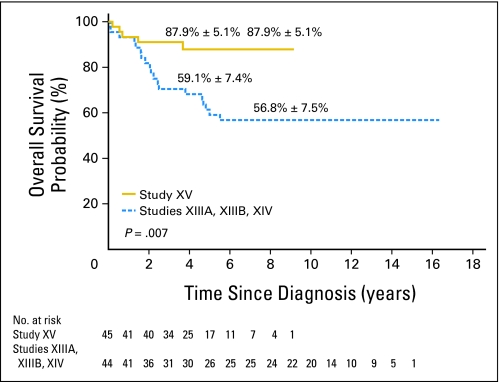
Results: The 89 older adolescents were significantly more likely to have T-cell ALL, the t(4;11)(MLL-AF4), and detectable minimal residual disease during or at the end of remission induction; they were less likely to have the t(12;21)(ETV6-RUNX1) compared with younger patients. In the first three studies, the 44 older adolescents had significantly poorer event-free survival and overall survival than the 403 younger patients. This gap in prognosis was abolished in study XV: event-free survival rates at 5 years were 86.4% ± 5.2% (standard error) for the 45 older adolescents and 87.4% ± 1.7% for the 453 younger patients; overall survival rates were 87.9% ± 5.1% versus 94.1% ± 1.2%, respectively.
Conclusion: Most older adolescents with ALL can be cured with risk-adjusted intensive chemotherapy without stem-cell transplantation.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
References
-
- Möricke A, Reiter A, Zimmermann M, et al. Risk-adjusted therapy of acute lymphoblastic leukemia can decrease treatment burden and improve survival: Treatment results of 2169 unselected pediatric and adolescent patients enrolled in the trial ALL-BFM 96. Blood. 2008;111:4477–4489. - PubMed
-
- Conter V, Aricò M, Basso G, et al. Long-term results of the Italian Association of Pediatric Hematology and Oncology (AIEOP) studies 82, 87, 88, 91 and 95 for childhood acute lymphoblastic leukemia. Leukemia. 2010;24:255–264. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
