

Review
doi: 10.1259/bjr/31861984.
Clinical presentations and imaging findings of neuroblastoma beyond abdominal mass and a review of imaging algorithm
Affiliations
- PMID: 21172969
- PMCID: PMC3473807
- DOI: 10.1259/bjr/31861984
Item in Clipboard
Review
Clinical presentations and imaging findings of neuroblastoma beyond abdominal mass and a review of imaging algorithm
Br J Radiol.
2011 Jan.
Abstract
Neuroblastoma is one of the most common malignant neoplasms in childhood. The most common clinical presentation of this tumour is abdominal mass. However, affected children may have various clinical presentations as a result of disseminated metastatic disease or associated paraneoplastic syndromes at the time of diagnosis. In this article we have outlined the imaging findings in seven patients with "extra-abdominal" presentation of neuroblastoma and the pitfalls in making the correct diagnosis. The purpose of this pictorial review is to alert the general radiologist to the possible presentations of this common childhood malignancy to derive early detection and diagnosis.
Figures

Right adrenal neuroblastoma in a 6-year-old boy who presented with left shoulder pain, anaemia and raised erythrocyte sedimentation rate (ESR). He was initially misdiagnosed as having juvenile idiopathic arthropathy. (a) Plain radiograph. When compared with the normal right side there is periarticular osteopenia of the left shoulder involving the clavicle (black arrow) and scapula (white arrow). (b) Coronal fat-saturation T2 weighted image of left shoulder shows multifocal increased marrow signal in the lateral end of the clavicle (black arrow), the scapula (white arrow) and the proximal humerus (arrowhead). A small amount of joint effusion is also evident. (c) Transverse ultrasound image of the abdomen shows a large heterogeneous mass at the right adrenal bed (M). It was confirmed as neuroblastoma after ultrasound-guided biopsy. (d) Contrast-enhanced axial CT image shows a large, poorly enhancing soft-tissue mass with classical vascular encasement of both renal arteries (black arrows) and right renal vein (white arrow).
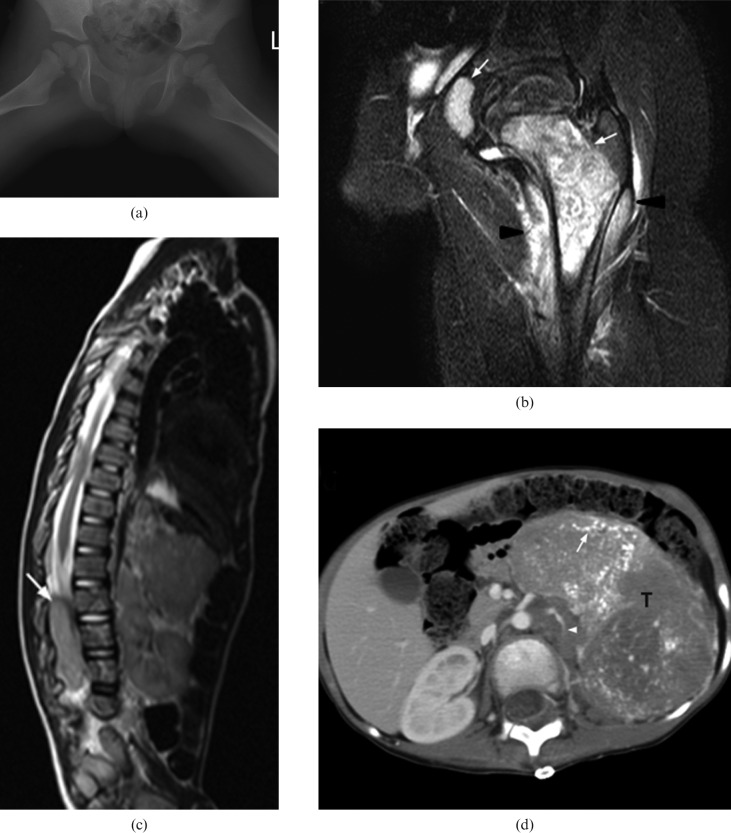
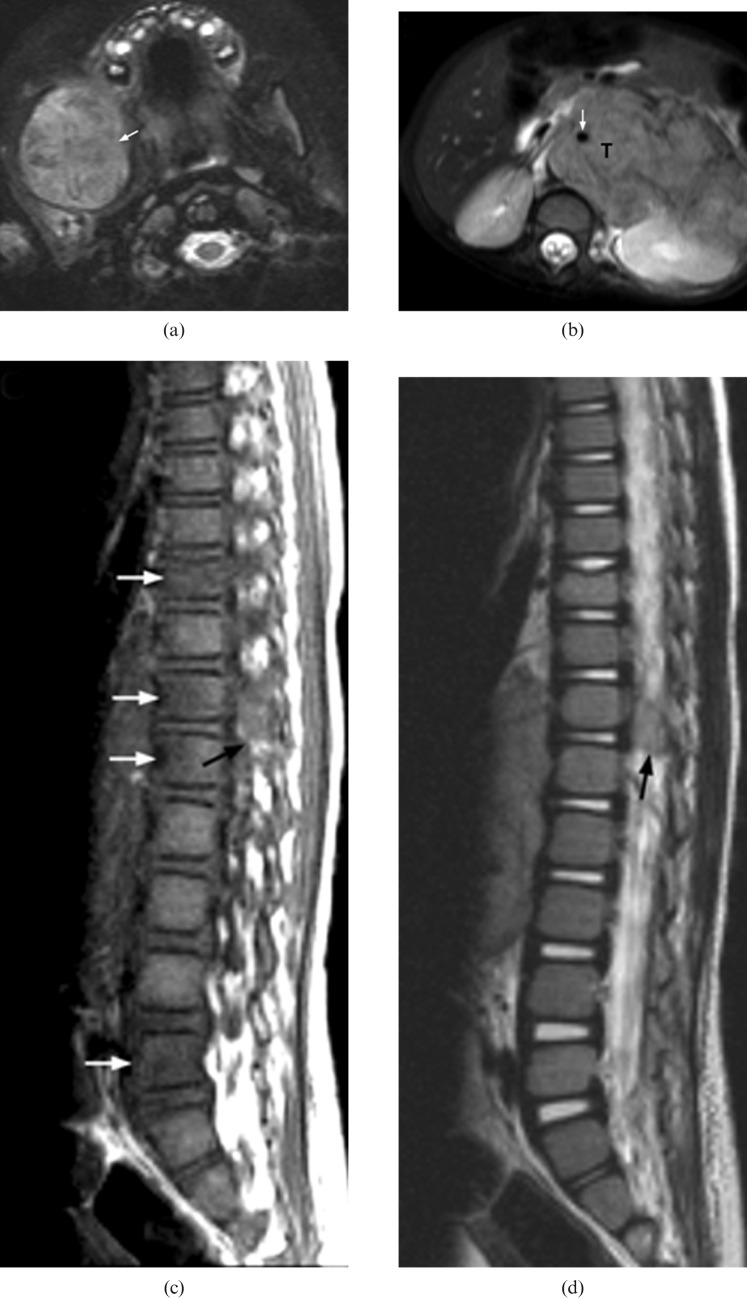
A 3-year-old boy with Stage IV neuroblastoma who presented with left hip pain, limp and fever. A blood test showed elevated chronic reactive protein (CRP). He was initially misdiagnosed as having septic arthritis. (a) Plain radiography of both hips shows no obvious bony destruction of the left proximal femur when compared with the asymptomatic right side. (b) Coronal MR T2 weighted image with fat saturation of the left hip reveals marked T2 hyperintense signal of proximal femoral metaphysic and acetablum (white arrows) together with signal change in the surrounding muscle (arrow heads). This was misinterpreted as osteomyelitis at the initial study. (c) MRI of the spine and abdomen shows distal cord and cauda equina compression by a large abdominal soft-tissue mass with intraspinal extension (white arrow). (d) Contrast-enhanced axial CT image shows a large heterogeneously enhancing soft-tissue mass (T) with extensive intratumoural calcifications (white arrow) in the left side abdomen. The left kidney (not shown) is displaced inferiorly and the left renal vein (arrowhead) is encased. Ultrasound biopsy confirmed neuroblastoma.
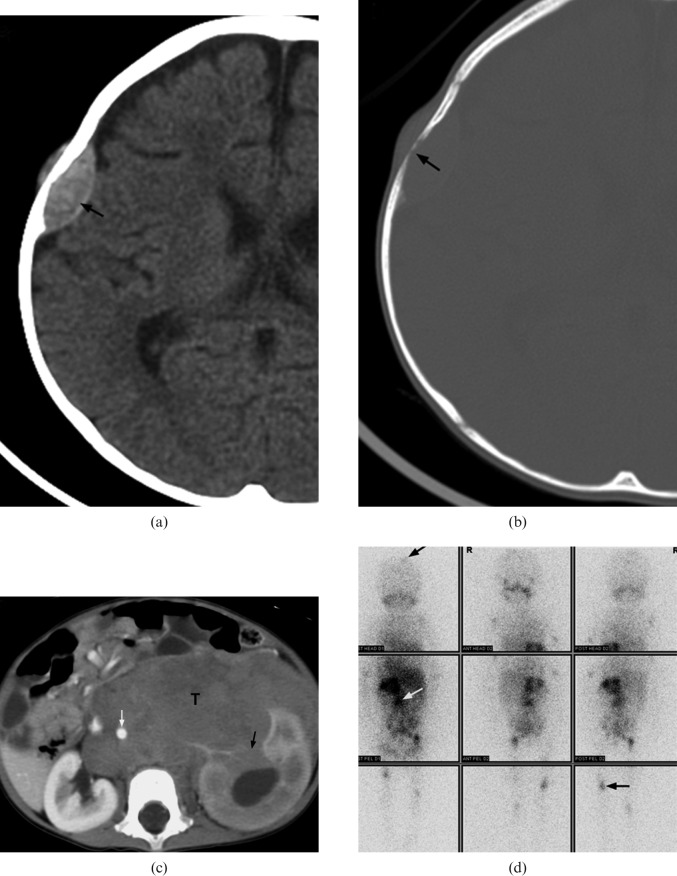
A 14-month-old girl with Stage IV neuroblastoma who presented with scalp nodules and on/off fever for two weeks. (a,b) Axial CT of brain demonstrates a lentiform soft-tissue mass in right parietal bone (black arrow) associated with bony erosion. (c) Contrast-enhanced axial CT image of abdomen shows a large soft-tissue mass (T) at the left sided retroperitoneal space. The tumour encases the abdominal aorta (white arrow) and invades the left kidney (black arrow). (d) Metaiodobenzylguanidine scintigraphy demonstrates multiple foci of abnormal tracer uptake (arrows) in the abdomen, skull and appendiceal skeleton.
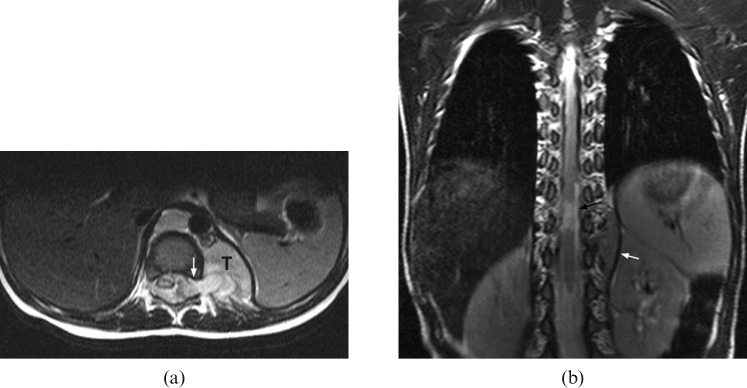
An 8-month-old boy with Stage III neuroblastoma who presented with diarrhoea for 5 days and was treated for gastroenteritis. Subsequently, he was found, by the mother, to have deterioration in standing power. (a) Axial T2 weighted MRI shows compression of the cord by a left paravertebral tumour (T) with intraspinal extension via the neural foramina (white arrow). (b) Follow-up coronal T2 weighted MRI reveals residual small left paravertebral tumour after completed treatment (white arrow). There is a short segment of myelomalacia (black arrow) at the distal cord. The patient suffers from a persistent neurological deficit.
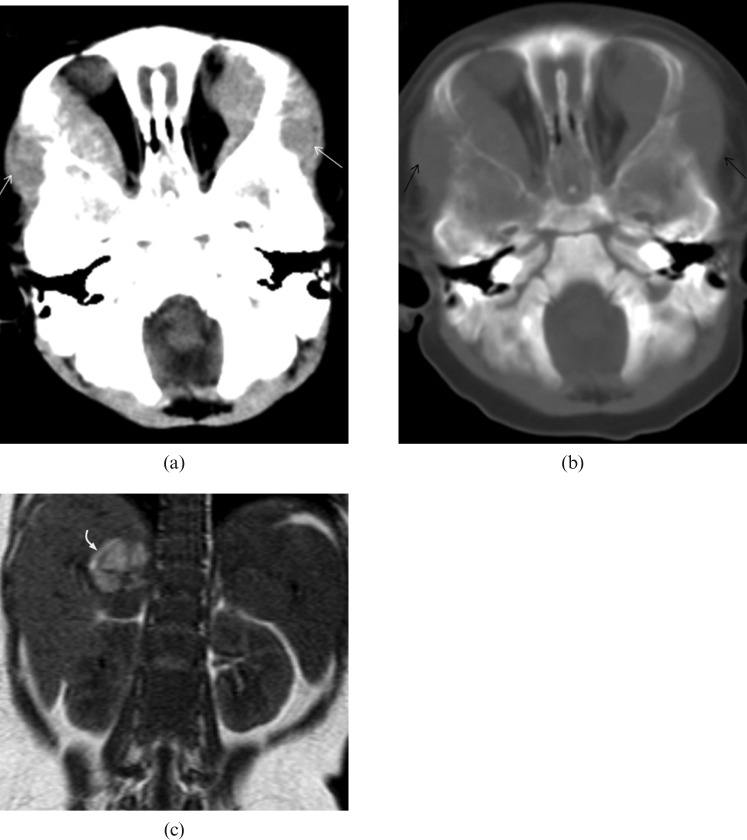
Stage IV neuroblastoma in a 7-month-old girl who presented with watery eye discharge and orbital swelling for 10 days. (a,b) CT image of the brain demonstrates bilateral intraorbital soft-tissue masses (white arrows) with bony orbit involvement (black arrows). It extends laterally into the subcutaneous soft tissues. (c) Coronal T1 weighted MRI shows a heterogeneous mass in which the high signal intensity area corresponds to tumoural haemorrhage (curved arrow).
Stage IV neuroblastoma in a 30-month-old girl who presented with right facial swelling. (a) Axial fat-saturation T2 weighted image shows a large tumour involving the body, angle and coronoid process of the right side of the mandible (arrow). (b) Axial T2 weighted MRI shows a large left adrenal tumour (T) encasing the abdominal aorta (white arrow). (c) Sagittal T1 weighted image and (d) T2 weighted image reveal direct extension of tumour into the spinal canal via the left T12/L1 intervertebral foramen (black arrow). There are multiple foci of abnormal signal intensity in the vertebral bodies at the level of T10, T12, L1 and L5 (white arrows).
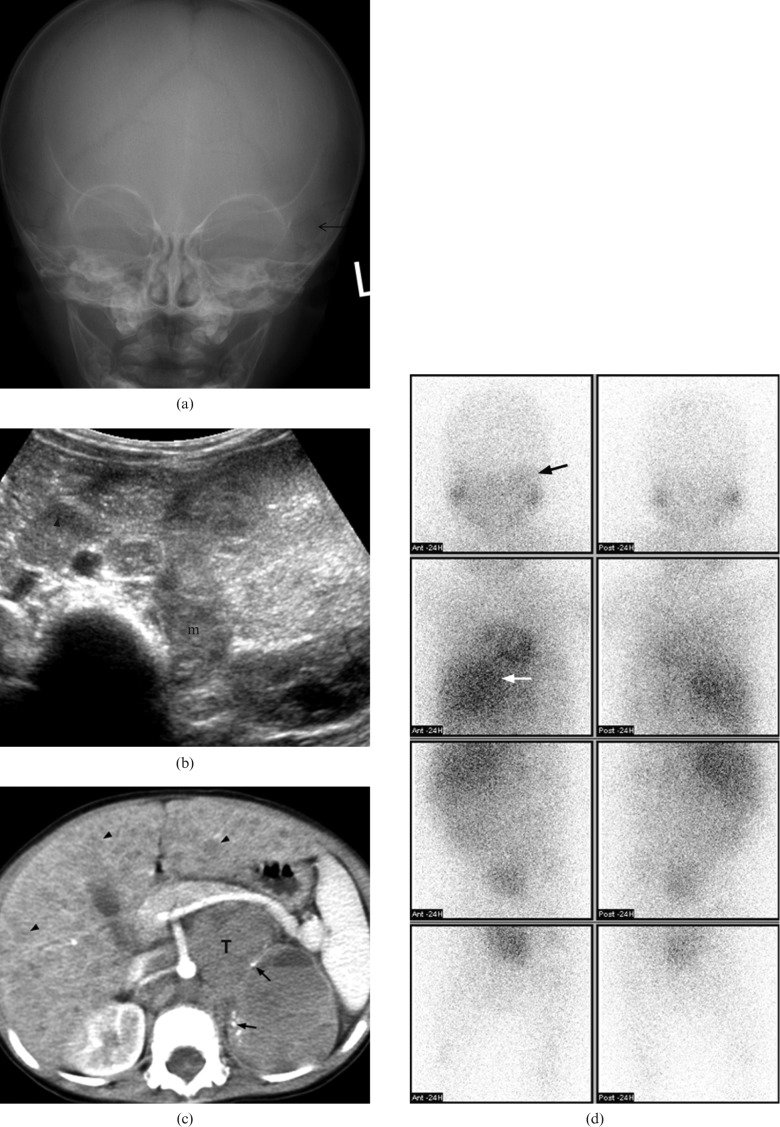
A 17-month-old boy with Stage IV neuroblastoma who presented with fatigue and periorbital swelling. (a) Plain radiography of the skull shows ill-defined lucency (arrow) over left periorbital bone. (b) Transverse ultrasound of abdomen shows an echogenic mass (m) at left adrenal bed with enlarged para-aortic lymph node (arrowhead). (c) Axial post-contrast CT of the abdomen shows a large mass (T) in the retroperitoneum with small amount of tumoural punctuate calcifications (arrows). The major vessels are encased. Diffuse liver metastases (black arrows) are also noted. (d) Metaiodobenzylguanidine scintigraphy shows increase in tracer uptake over left orbital region (black arrow). There is also intense uptake in the primary abdominal tumour (white arrow).
References
-
- David R, Lamki N, Fan S, Singleton EB, Eftekhari F, Shirkhoda A, et al. The many faces of neuroblastoma. Radiographics 1989;9:859–82 - PubMed
-
- Maris JM, Hogarty MD, Bagatell R, Cohn SL. Neuroblastoma. Lancet 2007;369:2106–20 - PubMed
-
- De Bernardi B, Nicolas B, Boni L, Indolfi P, Carli M, Cordero DiMontezemolo L, et al. Disseminated neuroblastoma in children older than one year at diagnosis: comparable results with three consecutive high-dose protocols adopted by the Italian Co-Operative Group for Neuroblastoma. J Clin Oncol 2003;21:1592–601 - PubMed
-
- Lonergan GJ, Schwab CM, Suarez ES, Carlson CL. Neuroblastoma, ganglioneuroblastoma, and ganglioneuroma: radiologic-pathologic correlation. Radiographics 2002;22:911–34 - PubMed
-
- Lanzkowsky P. Neuroblastoma. In: Lanzkowsky P, editor. Annual of pediatric hematology and oncology. 4 edn. London: Elsevier Academic Press, 2005::530–2
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
