

Editorial
doi: 10.1213/ANE.0b013e3181fec9a3.
Intraoperative methadone: rediscovery, reappraisal, and reinvigoration?
- PMID: 21173206
- PMCID: PMC3689220
- DOI: 10.1213/ANE.0b013e3181fec9a3
Item in Clipboard
Editorial
Intraoperative methadone: rediscovery, reappraisal, and reinvigoration?
Anesth Analg.
2011 Jan.
No abstract available
Conflict of interest statement
Conflict of interest: None
Figures
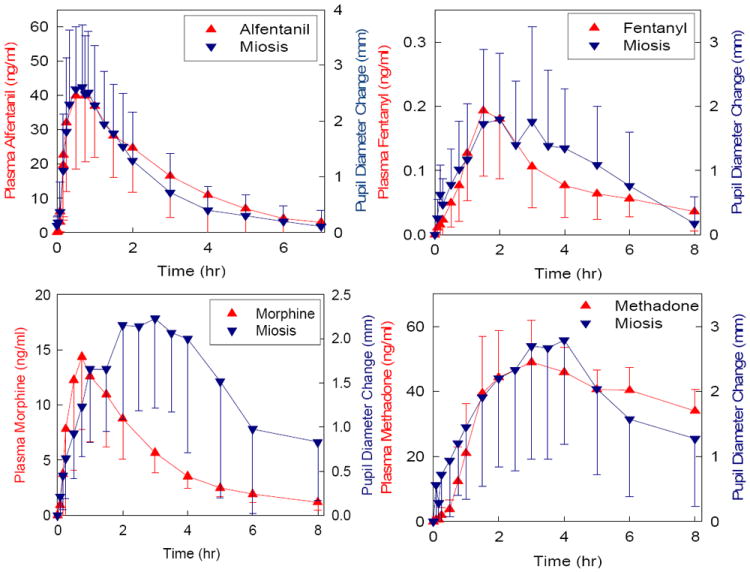
Relationship between opioid plasma concentration and onset of effect. Opioid effects was determined by pupil diameter change (miosis). Results are shown for alfentanil, fentanyl, methadone and morphine. Redrawn with permission.-
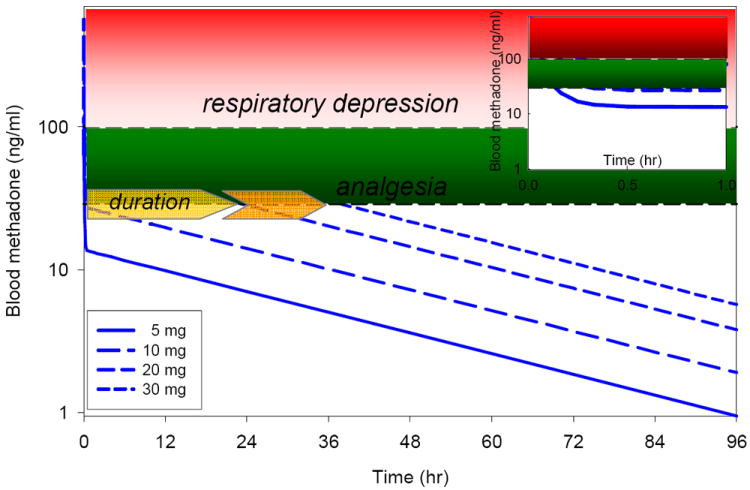
Relationship between methadone dose and duration of effect. Simulated methadone blood concentrations vs time are based on the pharmacokinetic parameters of Gourlay et al, as are the minimal effective analgesic methadone concentration (approximately 30 ng/ml), and the threshold for significant (5-6 breaths/min) respiratory depression (approximately 100 ng/ml). Data are shown for intravenous bolus methadone doses of 5, 10, 20 and 30 mg. Estimated duration of analgesia for these doses is approximately <0.5, <0.5, 24 and 36 hr. Duration of analgesia is governed by redistribution (and the redistribution half-life of approximately 5 min) for the 5 and 10 mg doses, but by elimination (and the elimination half-life of approximately 30 hr) for the larger doses. The inset shows plasma concentrations for the first hr after dosing. Due to rapid redistribution, anticipated respiratory depression would be less than 30-45 min, even at the higher single bolus doses.
Comment on
-
Intraoperative methadone improves postoperative pain control in patients undergoing complex spine surgery.Anesth Analg. 2011 Jan;112(1):218-23. doi: 10.1213/ANE.0b013e3181d8a095. Epub 2010 Apr 24. Anesth Analg. 2011. PMID: 20418538 Clinical Trial.
References
-
- Brennan F, Carr DB, Cousins M. Pain management: a fundamental human right. Anesth Analg. 2007;105:205–21. - PubMed
-
- Moss E, Taverner T, Norton P, Lesser P, Cole P. A survey of postoperative pain management in fourteen hospitals in the UK. Acute Pain. 2005;7:13–20.
-
- Taylor A, Stanbury L. A review of postoperative pain management and the challenges. Curr Anaesthesia Critical Care. 2009;20:188–94.
-
- Kehlet H, Jensen TS, Woolf CJ. Persistent postsurgical pain: risk factors and prevention. Lancet. 2006;367:1618–25. - PubMed
-
- Rathmell JP, Wu CL, Sinatra RS, Ballantyne JC, Ginsberg B, Gordon DB, Liu SS, Perkins FM, Reuben SS, Rosenquist RW, Viscusi ER. Acute post-surgical pain management: a critical appraisal of current practice. Reg Anesth Pain Med. 2006;31(suppl 1):1–42. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
