

The cost-effectiveness and population outcomes of expanded HIV screening and antiretroviral treatment in the United States
- PMID: 21173412
- PMCID: PMC3173812
- DOI: 10.7326/0003-4819-153-12-201012210-00004
The cost-effectiveness and population outcomes of expanded HIV screening and antiretroviral treatment in the United States
Abstract
Background: Although recent guidelines call for expanded routine screening for HIV, resources for antiretroviral therapy (ART) are limited, and all eligible persons are not currently receiving treatment.
Objective: To evaluate the effects on the U.S. HIV epidemic of expanded ART, HIV screening, or interventions to reduce risk behavior.
Design: Dynamic mathematical model of HIV transmission and disease progression and cost-effectiveness analysis.
Data sources: Published literature.
Target population: High-risk (injection drug users and men who have sex with men) and low-risk persons aged 15 to 64 years in the United States.
Time horizon: Twenty years and lifetime (costs and quality-adjusted life-years [QALYs]).
Perspective: Societal.
Intervention: Expanded HIV screening and counseling, treatment with ART, or both.
Outcome measures: New HIV infections, discounted costs and QALYs, and incremental cost-effectiveness ratios.
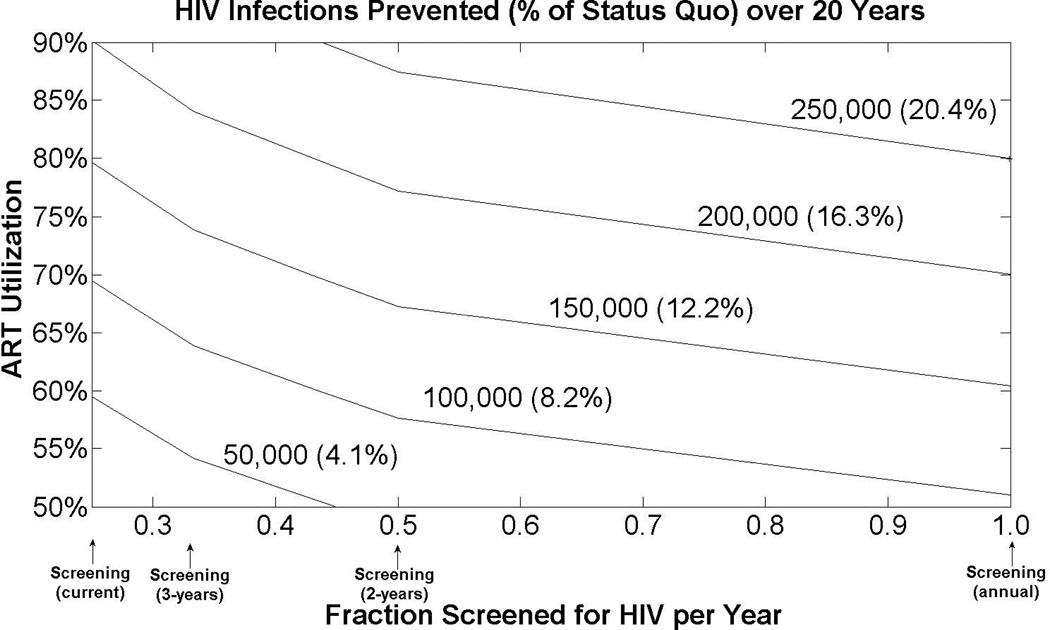
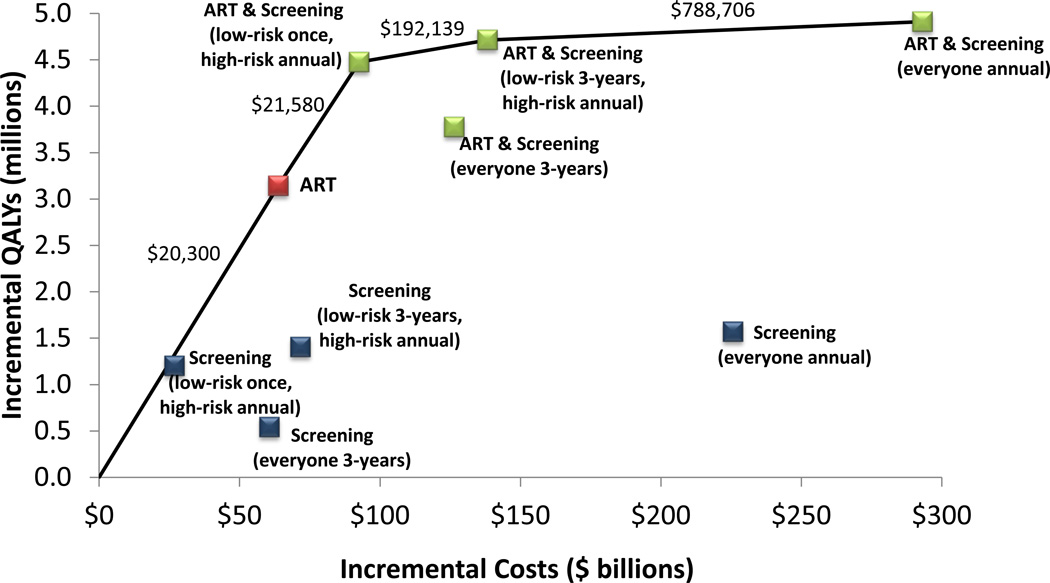
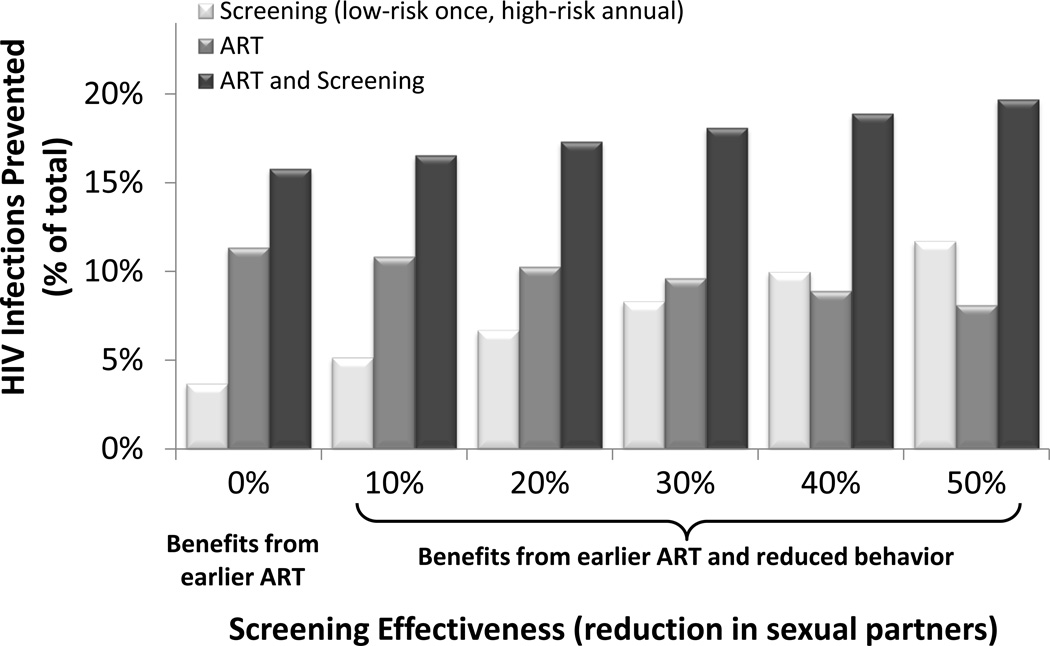
Results of base-case analysis: One-time HIV screening of low-risk persons coupled with annual screening of high-risk persons could prevent 6.7% of a projected 1.23 million new infections and cost $22,382 per QALY gained, assuming a 20% reduction in sexual activity after screening. Expanding ART utilization to 75% of eligible persons prevents 10.3% of infections and costs $20,300 per QALY gained. A combination strategy prevents 17.3% of infections and costs $21,580 per QALY gained.
Results of sensitivity analysis: With no reduction in sexual activity, expanded screening prevents 3.7% of infections. Earlier ART initiation when a CD4 count is greater than 0.350 × 10(9) cells/L prevents 20% to 28% of infections. Additional efforts to halve high-risk behavior could reduce infections by 65%.
Limitation: The model of disease progression and treatment was simplified, and acute HIV screening was excluded.
Conclusion: Expanding HIV screening and treatment simultaneously offers the greatest health benefit and is cost-effective. However, even substantial expansion of HIV screening and treatment programs is not sufficient to markedly reduce the U.S. HIV epidemic without substantial reductions in risk behavior.
Primary funding source: National Institute on Drug Abuse, National Institutes of Health, and Department of Veterans Affairs.
Figures
Comment in
-
Modeling the cost-effectiveness of health programs: HIV testing and early treatment in the USA.Future Microbiol. 2011 Jul;6(7):725-9. doi: 10.2217/fmb.11.63. Future Microbiol. 2011. PMID: 21797687
References
-
- Centers for Disease Control and Prevention (CDC) Estimates of New HIV Infections in the United States. [Accessed August 1, 2010];2008 http://www.cdc.gov/hiv/topics/surveillance/resources/factsheets/incidenc....
-
- Branson BM, Handsfield HH, Lampe MA, et al. Revised recommendations for HIV testing of adults, adolescents, and pregnant women in health-care settings. MMWR Recomm Rep. 2006;55(RR-14):1–17. - PubMed
-
- The National Institute of Mental Health (NIMH) Multisite HIV Prevention Trial Group. The NIMH Multisite HIV Prevention Trial: reducing HIV sexual risk behavior. Science. 1998;280(5371):1889–1894. - PubMed
-
- Kamb ML, Fishbein M, Douglas JM, Jr, et al. Efficacy of risk-reduction counseling to prevent human immunodeficiency virus and sexually transmitted diseases: a randomized controlled trial. Project RESPECT Study Group. JAMA. 1998;280(13):1161–1167. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous