

Postpartum hemorrhage resulting from uterine atony after vaginal delivery: factors associated with severity
- PMID: 21173641
- PMCID: PMC3319503
- DOI: 10.1097/AOG.0b013e318202c845
Postpartum hemorrhage resulting from uterine atony after vaginal delivery: factors associated with severity
Abstract
Objective: To identify factors associated with severity of postpartum hemorrhage among characteristics of women and their delivery, the components of initial postpartum hemorrhage management, and the organizational characteristics of maternity units.
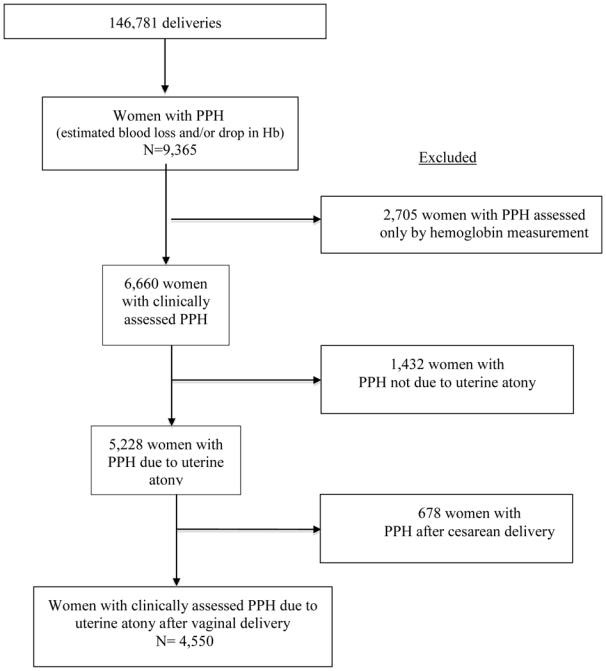
Methods: This population-based cohort study included women with postpartum hemorrhage due to uterine atony after vaginal delivery in 106 French hospitals between December 2004 and November 2006 (N=4,550). Severe postpartum hemorrhage was defined by a peripartum change in hemoglobin of 4 g/dL or more. A multivariable logistic model was used to identify factors independently associated with postpartum hemorrhage severity.
Results: Severe postpartum hemorrhage occurred in 952 women (20.9%). In women with postpartum hemorrhage, factors independently associated with severity were: primiparity; previous postpartum hemorrhage; previous cesarean delivery; cervical ripening; prolonged labor; and episiotomy; and delay in initial care for postpartum hemorrhage. Also associated with severity was 1) administration of oxytocin more than 10 minutes after postpartum hemorrhage diagnosis: 10-20 minutes after, proportion with severe postpartum hemorrhage 24.6% compared with 20.5%, adjusted OR 1.38, 95% CI 1.03-1.85; more than 20 minutes after, 31.8% compared with 20.5%, adjusted OR 1.86, CI 1.45-2.38; 2) manual examination of the uterine cavity more than 20 minutes after (proportion with severe postpartum hemorrhage 28.2% versus 20.7%, adjusted OR 1.83, 95% CI 1.42-2.35); 3) call for additional assistance more than 10 minutes after (proportion with severe postpartum hemorrhage 29.8% versus 24.8%, adjusted OR 1.61, 95% CI 1.23-2.12 for an obstetrician, and 35.1% compared with 29.9%, adjusted OR 1.51, 95% CI 1.14-2.00 for an anesthesiologist); 4) and delivery in a public non-university hospital. Epidural analgesia was found to be a protective factor against severe blood loss in women with postpartum hemorrhage.
Conclusion: Aspects of labor, delivery, and their management; delay in initial care; and place of delivery are independent risk factors for severe blood loss in women with postpartum hemorrhage caused by atony.
Level of evidence: II.
Comment in
-
Postpartum hemorrhage: becoming more evidence-based.Obstet Gynecol. 2011 Jan;117(1):3-5. doi: 10.1097/AOG.0b013e318202ec9a. Obstet Gynecol. 2011. PMID: 21173639 No abstract available.
References
-
- Brace V, Penney G, Hall M. Quantifying severe maternal morbidity: a Scottish population study. Bjog. 2004 May;111(5):481–4. - PubMed
-
- Callaghan WM, Mackay AP, Berg CJ. Identification of severe maternal morbidity during delivery hospitalizations, United States, 1991–2003. Am J Obstet Gynecol. 2008 Aug;199(2):133, e1–8. - PubMed
-
- Zhang WH, Alexander S, Bouvier-Colle MH, Macfarlane A. Incidence of severe pre-eclampsia, postpartum haemorrhage and sepsis as a surrogate marker for severe maternal morbidity in a European population-based study: the MOMS-B survey. Bjog. 2005;112(1):89–96. - PubMed
-
- Zwart JJ, Richters JM, Ory F, de Vries JI, Bloemenkamp KW, van Roosmalen J. Severe maternal morbidity during pregnancy, delivery and puerperium in the Netherlands: a nationwide population-based study of 371,000 pregnancies. Bjog. 2008 Jun;115(7):842–50. - PubMed
-
- Elbourne DR, Prendiville WJ, Carroli G, Wood J, McDonald S. Prophylactic use of oxytocin in the third stage of labour. Cochrane Database Syst Rev. 2001;(4):CD001808. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
