

Achievement of lipid targets with the combination of rosuvastatin and fenofibric Acid in patients with type 2 diabetes mellitus
- PMID: 21174145
- PMCID: PMC3070080
- DOI: 10.1007/s10557-010-6273-5
Achievement of lipid targets with the combination of rosuvastatin and fenofibric Acid in patients with type 2 diabetes mellitus
Abstract
Objective: The objective of this study was to assess the proportion of patients with type 2 diabetes mellitus (T2DM) attaining individual and combined targets of low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), triglycerides (TG), non-HDL-C, and apolipoprotein B (ApoB) after treatment with rosuvastatin (R) + fenofibric acid (FA) compared with corresponding-dose R monotherapy.
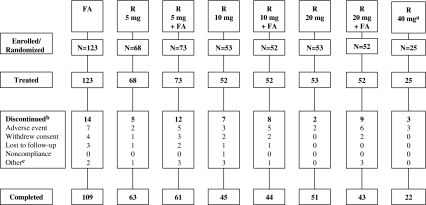
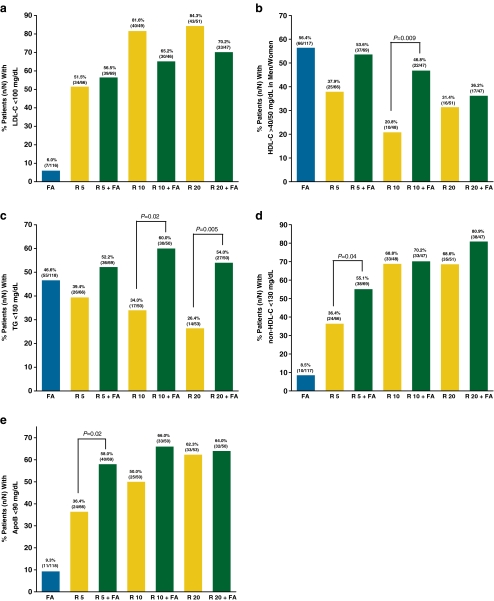
Methods: This post hoc analysis evaluated data from the T2DM subset of patients with mixed dyslipidemia (LDL-C ≥130 mg/dL, HDL-C <40/50 mg/dL in men/women, and TG ≥150 mg/dL) from 2 randomized studies. Patients included in the analysis (N = 456) were treated with R (5, 10, or 20 mg), FA 135 mg, or R (5, 10, or 20 mg) + FA 135 mg for 12 weeks. Attainment of LDL-C <100 mg/dL, HDL-C >40/50 mg/dL in men/women, TG <150 mg/dL, non-HDL-C <130 mg/dL, ApoB <90 mg/dL, and the combined targets of these parameters was assessed.
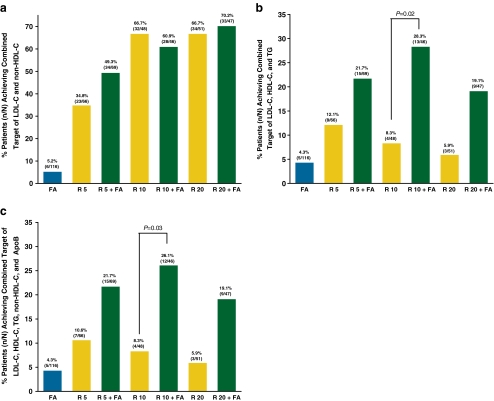
Results: Treatment with R + FA resulted in a significantly higher proportion of patients achieving optimal levels of HDL-C (46.8% vs. 20.8%, P = 0.009 for R 10 mg + FA), TG (60.0% vs. 34.0%, P = 0.02 for R 10 mg + FA; 54.0% vs. 26.4%, P = 0.005 for R 20 mg + FA), non-HDL-C (55.1% vs. 36.4%, P = 0.04 for R 5 mg + FA), ApoB (58.0% vs. 36.4%, P = 0.02 for R 5 mg + FA); and the combined targets of LDL-C, HDL-C, and TG (28.3% vs. 8.3%, P = 0.02 for R 10 mg + FA) and all 5 parameters (26.1% vs. 8.3%, P = 0.03 for R 10 mg + FA) than corresponding-dose R monotherapies.
Conclusions: A significantly greater proportion of T2DM patients achieved individual and combined lipid targets when treated with the combination of R + FA than corresponding-dose R monotherapies.
Trial registration: ClinicalTrials.gov NCT00300482 NCT00463606.
Figures
References
-
- Brunzell JD, Davidson M, Furburg CD, Goldberg RB, Howard BV, Stein JH, et al. Lipoprotein management in patients with cardiometabolic risk. Consensus statement from the American Diabetes Association and the American College of Cardiology Foundation. Diabetes Care. 2008;31:811–822. doi: 10.2337/dc08-9018. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
