

Variation in lymph node assessment after colon cancer resection: patient, surgeon, pathologist, or hospital?
- PMID: 21174232
- PMCID: PMC3568530
- DOI: 10.1007/s11605-010-1410-9
Variation in lymph node assessment after colon cancer resection: patient, surgeon, pathologist, or hospital?
Abstract
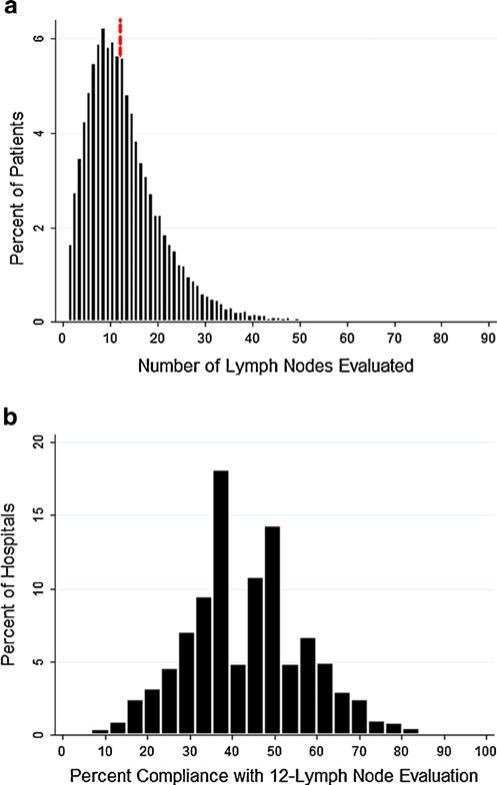
Background: Evaluation of ≥ 12 lymph nodes after colon cancer resection has been adopted as a hospital quality measure, but compliance varies considerably. We sought to quantify relative proportions of the variation in lymph node assessment after colon cancer resection occurring at the patient, surgeon, pathologist, and hospital levels.
Methods: The 1998-2005 Surveillance, Epidemiology, and End Results-Medicare database was used to identify 27,101 patients aged 65 years and older with Medicare parts A and B coverage undergoing colon cancer resection. Multilevel logistic regression was used to model lymph node evaluation as a binary variable (≥ 12 versus <12) while explicitly accounting for clustering of outcomes.
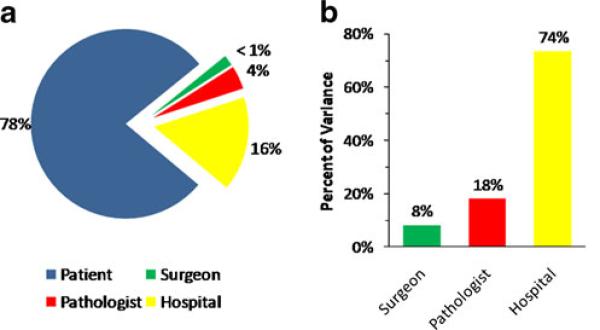
Results: Patients were treated by 4,180 distinct surgeons and 2,656 distinct pathologists at 1,113 distinct hospitals. The overall rate of 12-lymph node (12-LN) evaluation was 48%, with a median of 11 nodes examined per patient, and 33% demonstrated lymph node metastasis on pathological examination. Demographic and tumor-related characteristics such as age, gender, tumor grade, and location each demonstrated significant effects on rate of 12-LN assessment (all P < 0.05). The majority of the variation in 12-LN assessment was related to non-modifiable patient-specific factors (79%). After accounting for all explanatory variables in the full model, 8.2% of the residual provider-level variation was attributable to the surgeon, 19% to the pathologist, and 73% to the hospital.
Conclusion: Compliance with the 12-LN standard is poor. Variation between hospitals is larger than that between pathologists or surgeons. However, patient-to-patient variation is the largest determinant of 12-LN evaluation.
Figures
References
-
- Jemal A, Siegel R, Xu J, Ward E. Cancer statistics, 2010. CA: a cancer journal for clinicians. 2010;60:277–300. - PubMed
-
- Le Voyer TE, Sigurdson ER, Hanlon AL, et al. Colon cancer survival is associated with increasing number of lymph nodes analyzed: a secondary survey of intergroup trial INT-0089. J Clin Oncol. 2003;21:2912–9. - PubMed
-
- Swanson RS, Compton CC, Stewart AK, Bland KI. The prognosis of T3N0 colon cancer is dependent on the number of lymph nodes examined. Annals of surgical oncology. 2003;10:65–71. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
