

Review
doi: 10.2344/0003-3006-57.4.150.
Nausea, vomiting, and hiccups: a review of mechanisms and treatment
Affiliations
- PMID: 21174569
- PMCID: PMC3006663
- DOI: 10.2344/0003-3006-57.4.150
Item in Clipboard
Review
Nausea, vomiting, and hiccups: a review of mechanisms and treatment
Anesth Prog.
2010 Winter.
Abstract
Nausea, vomiting, and hiccups are troubling complications associated with sedation and general anesthesia. This article will review the basic pathophysiology of these events and current recommendations for their prevention and management.
Figures
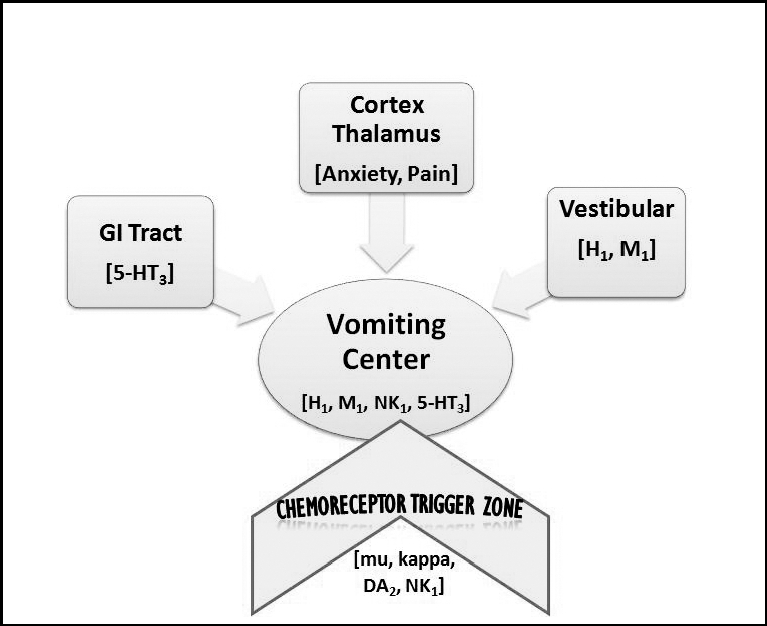
Pathophysiology of nausea and vomiting. Vomiting is caused by noxious stimulation of the vomiting center directly or indirectly via 1 or more of 4 additional sites: the gastrointestinal (GI) tract, the vestibular system, the chemoreceptor trigger zone, and higher centers in the cortex and thalamus. Once receptors are activated, neural pathways lead to the vomiting center, where emesis is initiated. Neural traffic originating in the GI tract travels along afferent fibers of cranial nerves IX (glossopharyngeal) and X (vagal). Antiemetic targets for drug interventions are predicated on their ability to block the illustrated receptor sites. Receptors illustrated along with their conventional ligands are as follows: H1 histamine, M1 acetylcholine, 5-HT3 serotonin, DA2 dopamine, NK1 (neurokinin) substance P, and mu/kappa opioids. Transmitter mediators in the cerebral cortex and thalamus are poorly understood, although cortical cannabinoid (CB1) pathways have been characterized.
References
-
- Guyton A. C., Hall J. E. Textbook of Medical Physiology. 11th ed. Philadelphia, Pa: Elsevier; 2006. pp. 823–824.
-
- Apfel C. C., Kranke P., Eberhart L. H. Comparison of surgical site and patient's history with a simplified risk score for the prediction of postoperative nausea and vomiting. Anaesthesia. 2004;59:1078–1082. - PubMed
-
- Apfel C. C. Postoperative nausea and vomiting. In: Miller R. D., Eriksson L. I., Fleisher L. A., et al., editors. Miller's Anesthesia. 7th ed. Philadelphia, Pa: Elsevier, Churchill Livingstone; 2009.
-
- Gupta A., Stierer T., Zuckerman R., et al. Comparison of recovery profile after ambulatory anesthesia with propofol, isoflurane, sevoflurane and desflurane: a systematic review. Anesth Analg. 2004;98:632–641. - PubMed
-
- Leslie K., Myles P. S., Chan M. T., et al. Risk factors for severe postoperative nausea and vomiting in a randomized trial of nitrous oxide-based vs nitrous oxide-free anaesthesia. Br J Anaesth. 2008;101:498–505. - PubMed
