

Cartilage in anterior cruciate ligament-reconstructed knees: MR imaging T1{rho} and T2--initial experience with 1-year follow-up
- PMID: 21177392
- PMCID: PMC3029884
- DOI: 10.1148/radiol.10101006
Cartilage in anterior cruciate ligament-reconstructed knees: MR imaging T1{rho} and T2--initial experience with 1-year follow-up
Abstract
Purpose: To longitudinally evaluate cartilage matrix changes by using magnetic resonance (MR) imaging T1(ρ) (T1 relaxation time in rotating frame) and T2 quantification and to study the relationship between meniscal damage and cartilage degeneration in anterior cruciate ligament (ACL)-reconstructed knees.
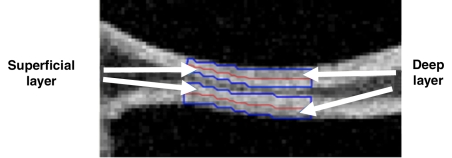
Materials and methods: This was an institutional review board-approved, HIPAA-compliant study. Informed consent was obtained. Twelve patients with acute ACL injuries were imaged with 3.0-T MR imaging at baseline (after injury and prior to ACL reconstruction) and 1 year after ACL reconstruction. Ten age-matched healthy subjects were studied as controls. Cartilage T1(ρ) and T2 were quantified in full thickness, superficial, and deep layers of defined subcompartments at baseline and follow-up in ACL-injured knees and were compared with measures acquired in matched regions of control knees. Meniscal lesions were graded by using modified subscores of the Whole-Organ Magnetic Resonance Imaging Score system.
Results: T1(ρ) values of the posterolateral tibial cartilage in ACL-injured knees were significantly elevated at baseline compared with T1(ρ)values of control knees and were not fully recovered at 1-year follow-up. T1(ρ) values of weight-bearing medial femorotibial cartilage in ACL-injured knees were significantly elevated at 1-year follow-up compared with those of control knees. No significant differences in T2 values between ACL-injured and control knees were found. Patients with lesions in the posterior horn of the medial meniscus showed a greater increase of T1(ρ) and T2 from baseline to follow-up in adjacent cartilage than patients without lesions in the medial meniscus.
Conclusion: Quantitative MR imaging T1(ρ) and T2 enable detection of changes in the cartilage matrix of ACL-reconstructed knees as early as 1 year after ACL reconstruction.
© RSNA, 2010
Figures













References
-
- Fu FH, Bennett CH, Ma CB, Menetrey J, Lattermann C. Current trends in anterior cruciate ligament reconstruction. II. Operative procedures and clinical correlations. Am J Sports Med 2000;28(1):124–130 - PubMed
-
- Ferretti A, Conteduca F, De Carli A, Fontana M, Mariani PP. Osteoarthritis of the knee after ACL reconstruction. Int Orthop 1991;15(4):367–371 - PubMed
-
- Daniel DM, Stone ML, Dobson BE, Fithian DC, Rossman DJ, Kaufman KR. Fate of the ACL-injured patient: a prospective outcome study. Am J Sports Med 1994;22(5):632–644 - PubMed
-
- Lohmander LS, Ostenberg A, Englund M, Roos H. High prevalence of knee osteoarthritis, pain, and functional limitations in female soccer players twelve years after anterior cruciate ligament injury. Arthritis Rheum 2004;50(10):3145–3152 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
