

Clinical effectiveness of elective single versus double embryo transfer: meta-analysis of individual patient data from randomised trials
- PMID: 21177530
- PMCID: PMC3006495
- DOI: 10.1136/bmj.c6945
Clinical effectiveness of elective single versus double embryo transfer: meta-analysis of individual patient data from randomised trials
Abstract
Objective: To compare the effectiveness of elective single embryo transfer versus double embryo transfer on the outcomes of live birth, multiple live birth, miscarriage, preterm birth, term singleton birth, and low birth weight after fresh embryo transfer, and on the outcomes of cumulative live birth and multiple live birth after fresh and frozen embryo transfers.
Design: One stage meta-analysis of individual patient data.
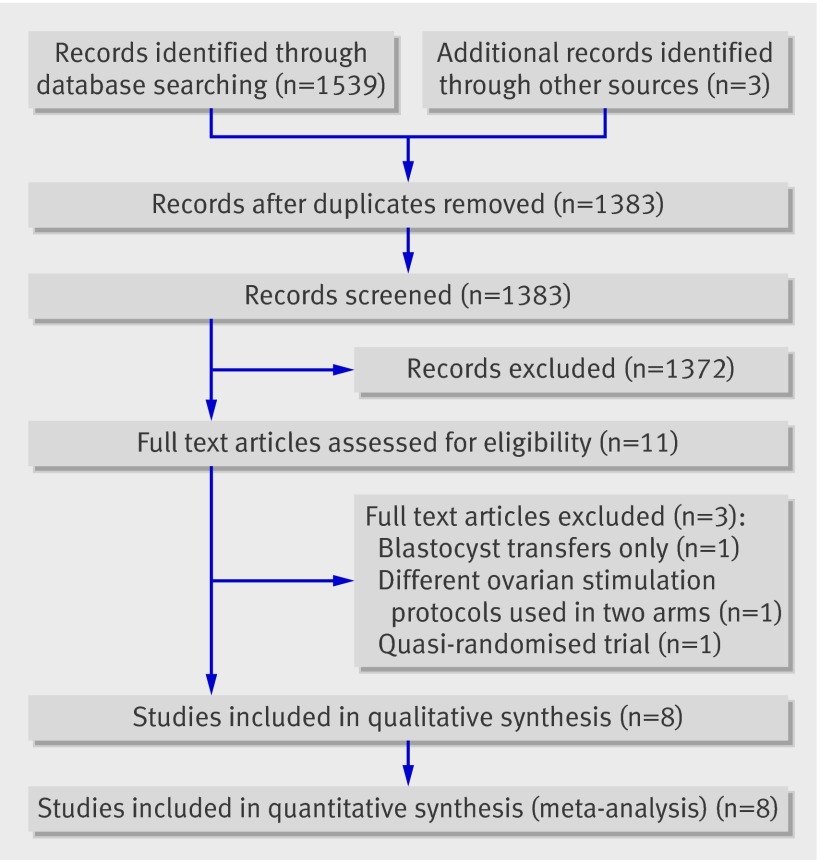
Data sources: A systematic review of English and non-English articles from Medline, Embase, and the Cochrane Central Register of Controlled Trials (up to 2008). Additional studies were identified by contact with clinical experts and searches of bibliographies of all relevant primary articles. Search terms included embryo transfer, randomised controlled trial, controlled clinical trial, single embryo transfer, and double embryo transfer. Review methods Comparisons of the clinical effectiveness of cleavage stage (day 2 or 3) elective single versus double embryo transfer after fresh or frozen in vitro fertilisation (IVF) or intracytoplasmic sperm injection (ICSI) treatments were included. Trials were included if the intervention differed only in terms of the intended number of embryos to be transferred. Trials that involved only blastocyst (day five) transfers were excluded.
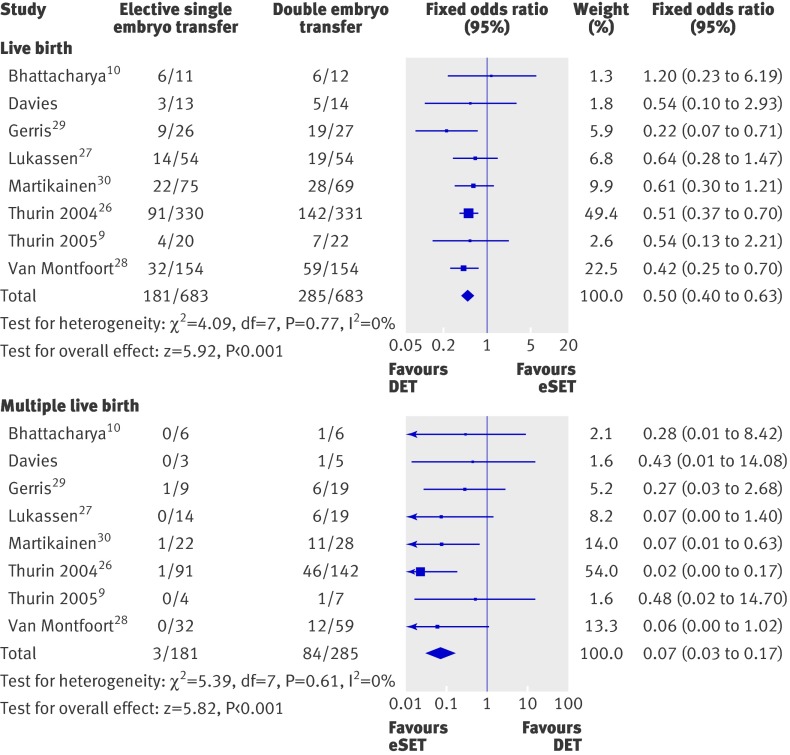
Results: Individual patient data were received for every patient recruited to all eight eligible trials (n=1367). A total of 683 and 684 women randomised to the single and double embryo transfer arms, respectively, were included in the analysis. Baseline characteristics in the two groups were comparable. The overall live birth rate in a fresh IVF cycle was lower after single (181/683, 27%) than double embryo transfer (285/683, 42%) (adjusted odds ratio 0.50, 95% confidence interval 0.39 to 0.63), as was the multiple birth rate (3/181 (2%) v 84/285 (29%)) (0.04, 0.01 to 0.12). An additional frozen single embryo transfer, however, resulted in a cumulative live birth rate not significantly lower than the rate after one fresh double embryo transfer (132/350 (38%) v 149/353 (42%) (0.85, 0.62 to 1.15), with a minimal cumulative risk of multiple birth (1/132 (1%) v 47/149 (32%)). The odds of a term singleton birth (that is, over 37 weeks) after elective single embryo transfer was almost five times higher than the odds after double embryo transfer (4.93, 2.98 to 8.18).
Conclusions: Elective single embryo transfer results in a higher chance of delivering a term singleton live birth compared with double embryo transfer. Although this strategy yields a lower pregnancy rate than a double embryo transfer in a fresh IVF cycle, this difference is almost completely overcome by an additional frozen single embryo transfer cycle. The multiple pregnancy rate after elective single embryo transfer is comparable with that observed in spontaneous pregnancies.
Conflict of interest statement
Competing interests: All authors have completed the Unified Competing Interest form at
Figures
Comment in
-
Elective single versus double embryo transfer.BMJ. 2010 Dec 21;341:c7083. doi: 10.1136/bmj.c7083. BMJ. 2010. PMID: 21177531 No abstract available.
References
-
- Bergh C. Single embryo transfer: a mini review. Hum Reprod 2005;20:323-7. - PubMed
-
- Gerris JM. Single embryo transfer and IVF/ICSI outcome: a balanced appraisal. Hum Reprod Update 2005;11:105-21. - PubMed
-
- Thurin Kjellberg A, Carlsson P, Bergh C. Randomized single versus double embryo transfer: obstetric and paediatric outcome and a cost-effectiveness analysis. Hum Reprod 2006;21:210-6. - PubMed
-
- De Mouzon J, Goossens V, Bhattacharya S, Castilla JA, Ferraretti AP, Korsak V, et al, and The European IVF-monitoring (EIM) Consortium, for the European Society of Human Reproduction and Embryology (ESHRE). Assisted reproductive technology in Europe, 2006: results generated from European registers by ESHRE. Hum Reprod 2010;25:1851-62. - PubMed
-
- Vilska S, Tiitinen A, Hyden-Granskog C, Hovatta O. Elective transfer of one embryo results in an acceptable pregnancy rate and eliminates the risk of multiple birth. Hum Reprod 1999;14:2392-5. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources