

Photodynamic therapy of tumors can lead to development of systemic antigen-specific immune response
- PMID: 21179470
- PMCID: PMC3001867
- DOI: 10.1371/journal.pone.0015194
Photodynamic therapy of tumors can lead to development of systemic antigen-specific immune response
Abstract
Background: The mechanism by which the immune system can effectively recognize and destroy tumors is dependent on recognition of tumor antigens. The molecular identity of a number of these antigens has recently been identified and several immunotherapies have explored them as targets. Photodynamic therapy (PDT) is an anti-cancer modality that uses a non-toxic photosensitizer and visible light to produce cytotoxic reactive oxygen species that destroy tumors. PDT has been shown to lead to local destruction of tumors as well as to induction of anti-tumor immune response.
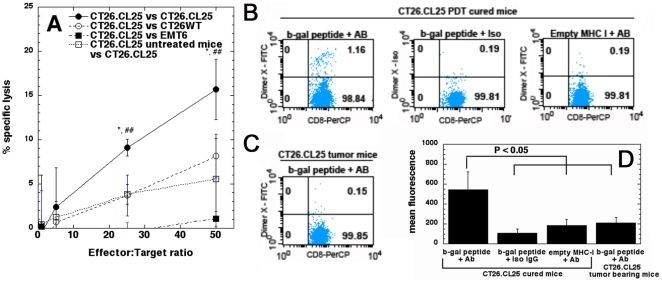
Methodology/principal findings: We used a pair of equally lethal BALB/c colon adenocarcinomas, CT26 wild-type (CT26WT) and CT26.CL25 that expressed a tumor antigen, β-galactosidase (β-gal), and we treated them with vascular PDT. All mice bearing antigen-positive, but not antigen-negative tumors were cured and resistant to rechallenge. T lymphocytes isolated from cured mice were able to specifically lyse antigen positive cells and recognize the epitope derived from beta-galactosidase antigen. PDT was capable of destroying distant, untreated, established, antigen-expressing tumors in 70% of the mice. The remaining 30% escaped destruction due to loss of expression of tumor antigen. The PDT anti-tumor effects were completely abrogated in the absence of the adaptive immune response.
Conclusion: Understanding the role of antigen-expression in PDT immune response may allow application of PDT in metastatic as well as localized disease. To the best of our knowledge, this is the first time that PDT has been shown to lead to systemic, antigen- specific anti-tumor immunity.
Conflict of interest statement
Figures





References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
