

Current status of antiviral therapy for hepatitis B
- PMID: 21180515
- PMCID: PMC3002488
- DOI: 10.1177/1756283X08093944
Current status of antiviral therapy for hepatitis B
Erratum in
- Therap Adv Gastroenterol. 2008 Sep;1(2):143
Abstract
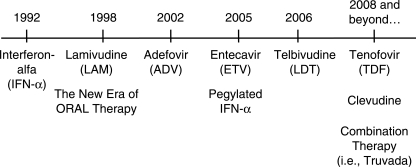
Chronic hepatitis B (CHB) is a major public health problem affecting up to 400 million people globally. Complications of CHB including liver failure and hepatocellular carcinoma result in 1.2 million deaths per year, making CHB the 10th leading cause of mortality worldwide. The natural history of CHB is variable and complex. The past decade witnessed important developments for the therapy of hepatitis B and marked the new era of oral therapy. The ultimate goal of CHB therapy is to arrest the progression of liver injury and to prevent the development of liver failure and hepatocellular carcinoma. Currently, six agents are approved for the treatment of CHB. Each of these agents, given as monotherapy, has been shown to produce virological, biochemical, and histological benefits for both HBeAg positive and negative CHB. There are, however, limitations in spite of their efficacy. The significant side-effect profile of interferon, for example, limits its long-term use. The approved oral agents are tolerable with prolonged use but drug resistance could limit long-term monotherapy. To date, combination therapy with nucleoside analogue and pegylated interferon or two nucleos(t)ide analogues given for one year does not show superiority in durability of response compared to monotherapy. Ongoing research effort is critical to identify the ideal hepatitis B therapy that is safe, effective, and produces durable response with a finite course of therapy. It is equally important to conduct a well designed, prospective natural history study to identify predictors of disease progression. This will accurately guide treatment strategy for this important disease.
Keywords: Hepatitis B virus; drug resistance; nucleos(t)ide analogues; pegylated interferon.
Figures

References
-
- Alward W.L., McMahon B.J., Hall D.B., Heyward W.L., Francis D.P., Bender T.R. (1985) The long-term serological course of asymptomatic hepatitis B virus carriers and the development of primary hepatocellular carcinoma. J Infect Dis 151(4):604–609 - PubMed
-
- Arora G., Keeffe E.B. (2007) Chronic hepatitis B with advanced fibrosis or cirrhosis: impact of antiviral therapy. Rev Gastroenterol Disord 7(2):63–73 - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
