

Noninvasive assessment of burn wound severity using optical technology: a review of current and future modalities
- PMID: 21185123
- PMCID: PMC3131405
- DOI: 10.1016/j.burns.2010.11.012
Noninvasive assessment of burn wound severity using optical technology: a review of current and future modalities
Abstract
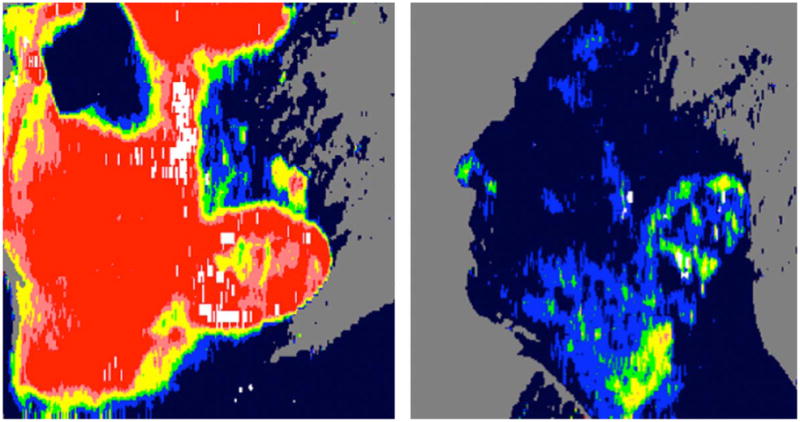
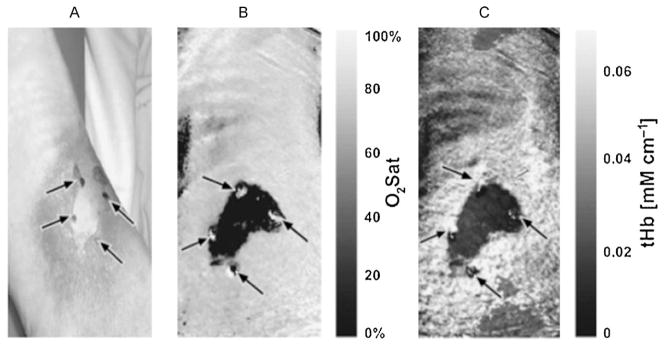
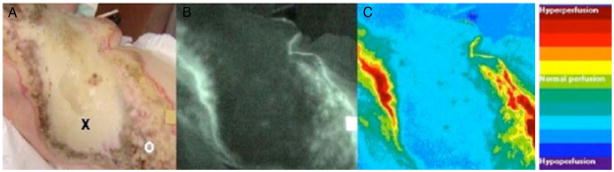
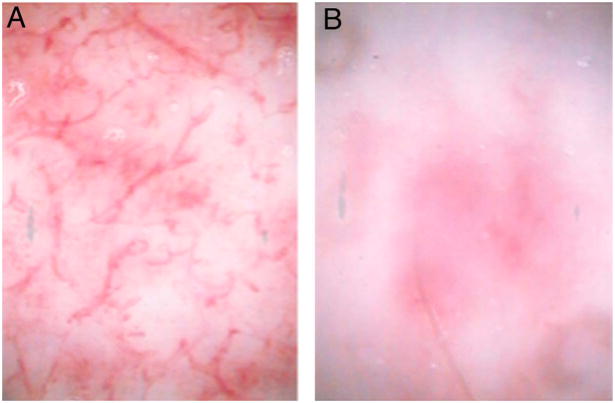
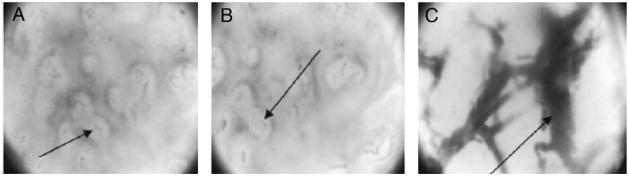
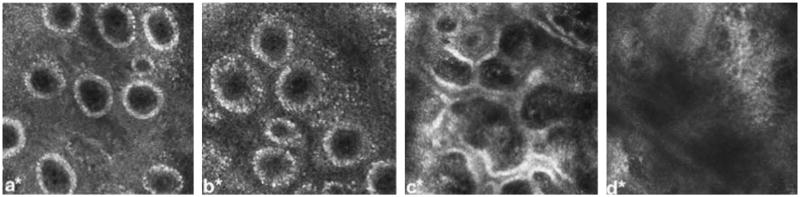
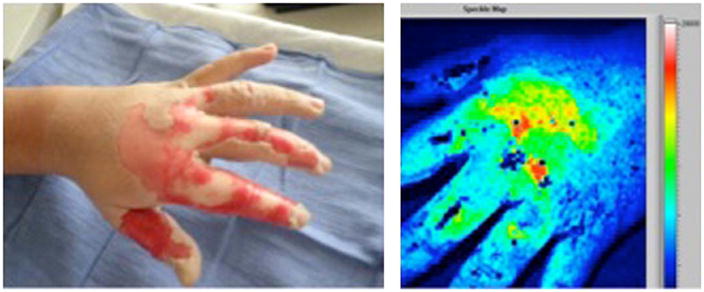
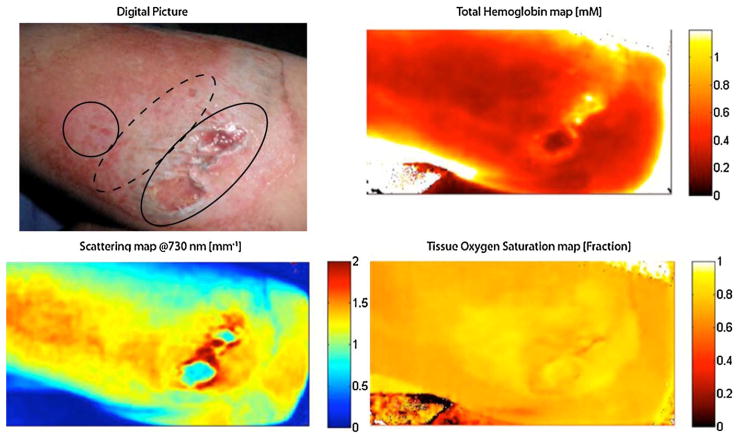
Clinical examination alone is not always sufficient to determine which burn wounds will heal spontaneously and which will require surgical intervention for optimal outcome. We present a review of optical modalities currently in clinical use and under development to assist burn surgeons in assessing burn wound severity, including conventional histology/light microscopy, laser Doppler imaging, indocyanine green videoangiography, near-infrared spectroscopy and spectral imaging, in vivo capillary microscopy, orthogonal polarization spectral imaging, reflectance-mode confocal microscopy, laser speckle imaging, spatial frequency domain imaging, photoacoustic microscopy, and polarization-sensitive optical coherence tomography.
Copyright © 2010 Elsevier Ltd and ISBI. All rights reserved.
Conflict of interest statement
Dr. Anthony Durkin has a financial interest in Modulated Imaging Inc., a company with interests related to spatial field domain imaging (SFDI). Dr. Durkin is a cofounder of the company and owns equity interests in Modulated Imaging.
Figures
References
-
- Janzekovic Z. A new concept in the early excision and immediate grafting of burns. J Trauma. 1970;10(12):1103–8. - PubMed
-
- Cramer LM, McCormack RM, Carroll DB. Progressive partial excision and early grafting in lethal burns. Plast Reconstr Surg Transplant Bull. 1962;30:595–9. - PubMed
-
- Meeker IA, Snyder WH. Dermatome debridement and early grafting of extensive third degree burns in children. Surg Gynelcol Obstet. 1956;103(5):527–34. - PubMed
-
- Saffle JR. Practice guidelines for burn care. J Burn Care Rehabil. 2001;22(Suppl 1)
-
- Orgill DP. Excision and skin grafting of thermal burns. N Engl J Med. 2009;360(9):893–901. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
