

Risk for life-threatening cardiac events in patients with genotype-confirmed long-QT syndrome and normal-range corrected QT intervals
- PMID: 21185501
- PMCID: PMC3332533
- DOI: 10.1016/j.jacc.2010.07.038
Risk for life-threatening cardiac events in patients with genotype-confirmed long-QT syndrome and normal-range corrected QT intervals
Abstract
Objectives: This study was designed to assess the clinical course and to identify risk factors for life-threatening events in patients with long-QT syndrome (LQTS) with normal corrected QT (QTc) intervals.
Background: Current data regarding the outcome of patients with concealed LQTS are limited.
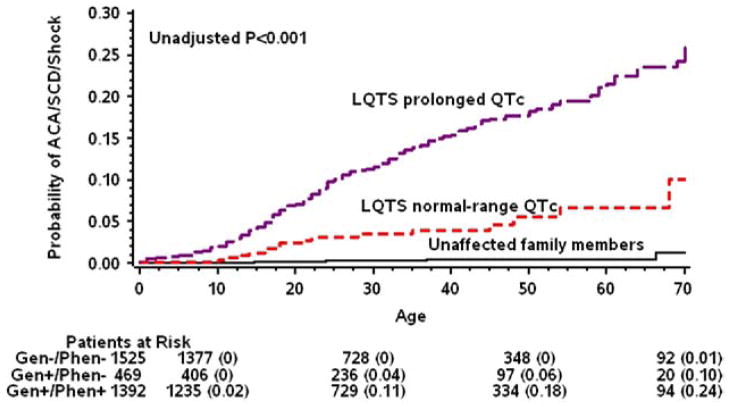
Methods: Clinical and genetic risk factors for aborted cardiac arrest (ACA) or sudden cardiac death (SCD) from birth through age 40 years were examined in 3,386 genotyped subjects from 7 multinational LQTS registries, categorized as LQTS with normal-range QTc (≤ 440 ms [n = 469]), LQTS with prolonged QTc interval (> 440 ms [n = 1,392]), and unaffected family members (genotyped negative with ≤ 440 ms [n = 1,525]).
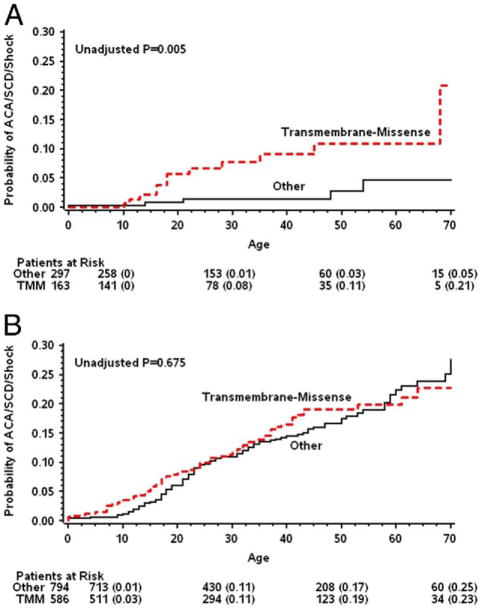
Results: The cumulative probability of ACA or SCD in patients with LQTS with normal-range QTc intervals (4%) was significantly lower than in those with prolonged QTc intervals (15%) (p < 0.001) but higher than in unaffected family members (0.4%) (p < 0.001). Risk factors ACA or SCD in patients with normal-range QTc intervals included mutation characteristics (transmembrane-missense vs. nontransmembrane or nonmissense mutations: hazard ratio: 6.32; p = 0.006) and the LQTS genotypes (LQTS type 1:LQTS type 2, hazard ratio: 9.88; p = 0.03; LQTS type 3:LQTS type 2, hazard ratio: 8.04; p = 0.07), whereas clinical factors, including sex and QTc duration, were associated with a significant increase in the risk for ACA or SCD only in patients with prolonged QTc intervals (female age > 13 years, hazard ratio: 1.90; p = 0.002; QTc duration, 8% risk increase per 10-ms increment; p = 0.002).
Conclusions: Genotype-confirmed patients with concealed LQTS make up about 25% of the at-risk LQTS population. Genetic data, including information regarding mutation characteristics and the LQTS genotype, identify increased risk for ACA or SCD in this overall lower risk LQTS subgroup.
Copyright © 2011 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures


Comment in
-
Genetic testing in subjects with no clinical abnormality: the tip of a huge iceberg.J Am Coll Cardiol. 2011 Jan 4;57(1):60-2. doi: 10.1016/j.jacc.2010.08.622. J Am Coll Cardiol. 2011. PMID: 21185502 No abstract available.
References
-
- Moss AJ, Schwartz PJ, Crampton RS, et al. The long QT syndrome. Prospective longitudinal study of 328 families. Circulation. 1991;84:1136–44. - PubMed
-
- Goldenberg I, Moss AJ. Long QT syndrome. J Am Coll Cardiol. 2008;51:2291–300. - PubMed
-
- Hobbs JB, Peterson DR, Moss AJ, et al. Risk of aborted cardiac arrest or sudden cardiac death during adolescence in the long-QT syndrome. JAMA. 2006;296:1249–54. - PubMed
-
- Sauer AJ, Moss AJ, McNitt S, et al. Long QT syndrome in adults. J Am Coll Cardiol. 2007;49:329–37. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
