

The prognosis for aphasia in stroke
- PMID: 21185744
- PMCID: PMC3117986
- DOI: 10.1016/j.jstrokecerebrovasdis.2010.09.009
The prognosis for aphasia in stroke
Abstract
Background: Aphasia is a disabling chronic stroke symptom, but the prognosis for patients presenting with aphasia in the hyperacute window has not been well characterized. The purpose of this study is to assess the prognosis for recovery of language function in subjects presenting with aphasia caused by ischemic stroke within 12 hours of symptom onset.
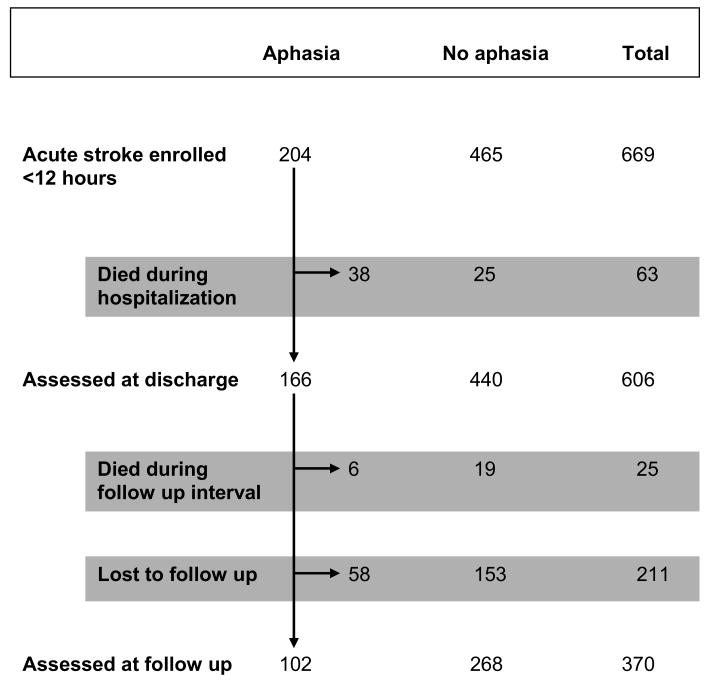
Methods: Subjects presenting with aphasia were identified from a prospective cohort study of 669 subjects presenting emergently with acute stroke. Subjects were characterized by demographics, serial clinical examinations, unenhanced computed tomography, and computed tomographic angiography. Aphasia severity was assessed by National Institutes of Health Stroke Scale (NIHSS) examinations performed at baseline, discharge, and 6 months. Demographic, clinical, and imaging factors were assessed for prognostic impact.
Results: Aphasia was present in 30% of subjects (n = 204). Of the 166 aphasic patients alive at discharge (median 5 days), aphasia improved in 57% and resolved in 38%. In the 102 aphasic subjects evaluated at 6 months, aphasia improved in 86% and completely resolved in 74% of subjects. Among aphasic subjects with "mild" stroke (initial NIHSS <5), aphasia resolved in 90% of subjects by 6 months. Factors significantly associated with better outcome included clinically and radiographically smaller strokes and lower prestroke disability.
Conclusions: The prognosis for full recovery of aphasia present in the hyperacute window is good. Radiographic and clinical markers indicating lesser extent of ischemia correlated to greater recovery. Given the excellent prognosis for language recovery in mild stroke, the net benefit of thrombolysis in such cases is uncertain.
Copyright © 2012 National Stroke Association. All rights reserved.
Conflict of interest statement
Conflicts of Interest/Disclosures:
Matthew B. Maas, MD- none.
Michael H. Lev, MD- is a speaker for GE Healthcare, Waukesha, WI; receives research support from GE Healthcare; and serves as a consultant for CoAxia, Maple Grove, MN, GE Healthcare, Waukesha, WI and Millennium Pharmaceuticals, Cambridge, MA.
Hakan Ay, MD- none.
Aneesh B. Singhal, MD- none.
David M. Greer, MD, MA- has served on the speaker's bureau for Boehringer-Ingelheim Pharmaceuticals, Ridgefield, CT.
Wade S. Smith, MD, PhD- owns stock and has stock options in Concentric Medical, Inc., Mountain View, CA, is a paid consultant for Concentric Medical, Inc., and has a research grant from Boerhinger-Ingelheim Pharmaceuticals, Ridgefield, CT.
Gordon J. Harris, PhD- none.
Elkan F. Halpern, PhD- none.
Walter J. Koroshetz, MD- none.
Karen L. Furie, MD, MPH- none.
References
-
- Ferro JM, Mariano G, Madureira S. Recovery from aphasia and neglect. Cerebrovasc Dis. 1999;9 5:6–22. - PubMed
-
- Brott T, Adams HP, Jr, Olinger CP, et al. Measurements of acute cerebral infarction: a clinical examination scale. Stroke. 1989;20:864–70. - PubMed
-
- Barber PA, Demchuk AM, Zhang J, Buchan AM. Validity and reliability of a quantitative computed tomography score in predicting outcome of hyperacute stroke before thrombolytic therapy. ASPECTS Study Group. Alberta Stroke Programme Early CT Score. Lancet. 2000;355:1670–4. - PubMed
-
- Ay H, Furie KL, Singhal A, Smith WS, Sorensen AG, Koroshetz WJ. An evidence-based causative classification system for acute ischemic stroke. Ann Neurol. 2005;58:688–97. - PubMed
-
- Ay H, Benner T, Arsava EM, et al. A computerized algorithm for etiologic classification of ischemic stroke: the Causative Classification of Stroke System. Stroke. 2007;38:2979–84. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
