

The effect of race and ethnicity on outcomes among patients in the intensive care unit: a comprehensive study involving socioeconomic status and resuscitation preferences
- PMID: 21187746
- PMCID: PMC3638889
- DOI: 10.1097/CCM.0b013e318206b3af
The effect of race and ethnicity on outcomes among patients in the intensive care unit: a comprehensive study involving socioeconomic status and resuscitation preferences
Abstract
Objective: We sought to determine whether race or ethnicity is independently associated with mortality or intensive care unit length of stay among critically ill patients after accounting for patients' clinical and demographic characteristics including socioeconomic status and resuscitation preferences.
Design: Historical cohort study of patients hospitalized in intensive care units.
Setting: Adult intensive care units in 35 California hospitals during the years 2001-2004.
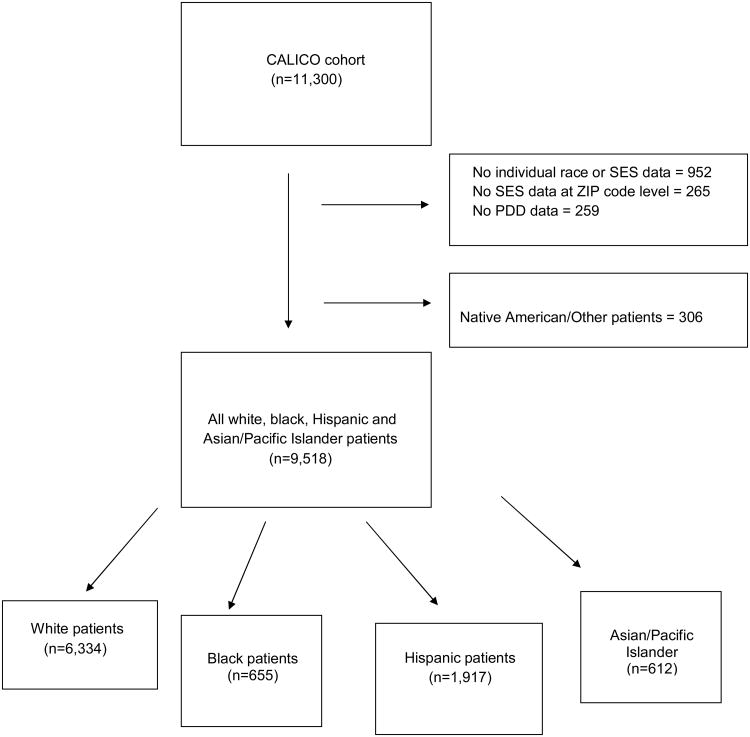
Patients: A total of 9,518 intensive care unit patients (6,334 white, 655 black, 1,917 Hispanic, and 612 Asian/Pacific Islander patients).
Measurements and main results: The primary outcome was risk-adjusted mortality and a secondary outcome was risk-adjusted intensive care unit length of stay. Crude hospital mortality was 15.9% among the entire cohort. Asian patients had the highest crude hospital mortality at 18.6% and black patients had the lowest at 15.0%. After adjusting for age and gender, Hispanic and Asian patients had a higher risk of death compared to white patients, but these differences were not significant after additional adjustment for severity of illness. Black patients had more acute physiologic derangements at intensive care unit admission and longer unadjusted intensive care unit lengths of stay. Intensive care unit length of stay was not significantly different among racial/ethnic groups after adjustment for demographic, clinical, and socioeconomic factors and do-not-resuscitate status. In an analysis restricted only to those who died, decedent black patients averaged 1.1 additional days in the intensive care unit (95% confidence interval, 0.26-2.6) compared to white patients who died, although this was not statistically significant.
Conclusions: Hospital mortality and intensive care unit length of stay did not differ by race or ethnicity among this diverse cohort of critically ill patients after adjustment for severity of illness, resuscitation status, socioeconomic status, insurance status, and admission type. Black patients had more acute physiologic derangements at intensive care unit admission and were less likely to have a do-not-resuscitate order. These results suggest that among intensive care unit patients, there are no racial or ethnic differences in mortality within individual hospitals. If disparities in intensive care unit care exist, they may be explained by differences in the quality of care provided by hospitals that serve high proportions of minority patients.
Figures
Comment in
-
Race and ethnicity in the intensive care unit: what do we know and where are we going?Crit Care Med. 2011 Mar;39(3):579-80. doi: 10.1097/CCM.0b013e31820a85be. Crit Care Med. 2011. PMID: 21330852 No abstract available.
References
-
- Smedley BD, SA, Nelson AR, et al. Unequal treatment: Confronting racial and ethnic disparities in health care. Washington, D.C.: Institute of Medicine; 2003. - PubMed
-
- Williams JF, Zimmerman JE, Wagner DP, Hawkins M, Knaus WA. African-American and white patients admitted to the intensive care unit: is there a difference in therapy and outcome? Crit Care Med. 1995;23:626–36. - PubMed
-
- Fisher E, GD, Skinner J, Bronner K. Health Care Spending, Quality and Outcomes: The Dartmouth Institute. 2009 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
